
This article has been verified for CPD. Click the button below to answer a few
short questions and download a form to be included in your CPD folder.

Chemical peels continue to be one of the most popular aesthetic treatments. With an ever-growing number of brands to choose from, Anna Baker explores the ingredients and formulations.
The term chemical peel is used to cover a growing number of in-clinic skin treatments, and at home options to treat a variety of different age-related skin concerns [1]. These treatments continue to sustain their popularity, reinforced by data from The Aesthetic Society (2019) ranking as the sixth most popular non-surgical treatment with 78,971 treatments performed [2].
The term chemical peel broadly refers to procedures which are chemically based, rejuvenating the face as well as the body, and can treat many cosmetic concerns such as mild-moderate acne with / without superficial scarring, signs of photo-ageing, textural irregularities (enlarged pores and rough skin), as well as areas of hyperpigmentation [3]. The common mechanism which underpins many chemical peel formulations is to elicit a level of stimulation in the skin to trigger healing, repair or collagen synthesis [4].
The mechanism of the ingredients in the chemical peel formulation can influence the depth and target structures for the formulation [5]. The formulations range from the concept of the ‘lunchtime peel’, which generally refers to formulations which offer chemical exfoliation and immediate brightening without desquamation, through to formulations which pass into deeper tissue planes stimulating an advanced anti-ageing response [6].
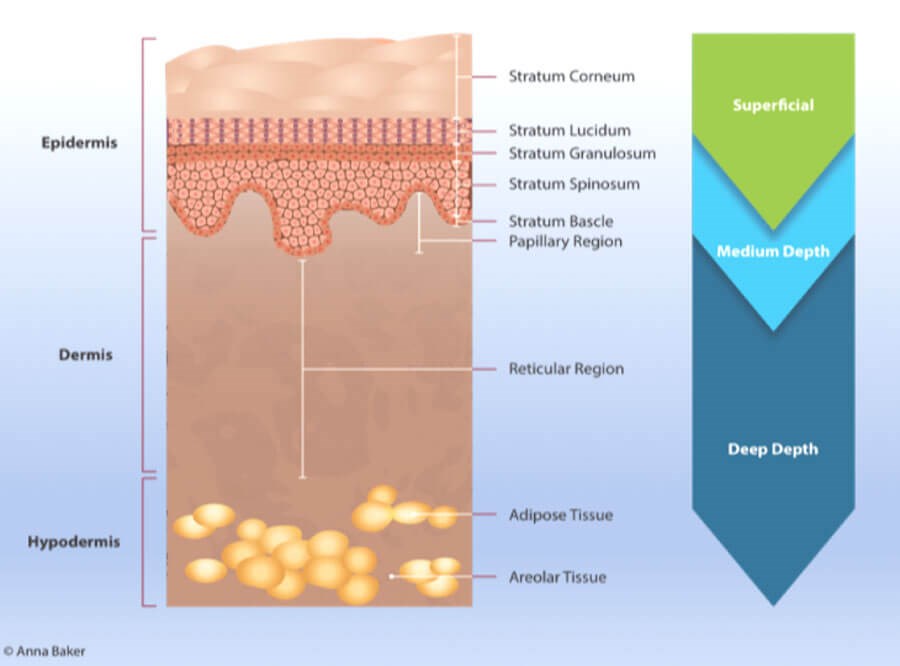
Cross section of the skin showing the layers (note: the stratum lucidum
is located on the soles of the feet and palms of the hands).
Chemical peel selection can be influenced by the clinician and patient’s preference, as well as individual professional scope of competence. Other important factors can include the nature and concentration of the peeling agent, number of applications, contact time on the skin, and varying degrees of desquamation [7].
While there is no formal or universally recognised classification to categorise the many brands of chemical peels available, it is generally accepted that peels can be categorised by their depth and therefore mode of action. This article will explore some of the commonly used ingredients (and formulations) but is not intended to be exhaustive in light of the increasing number of available formulations.
Clinical considerations
In the author’s opinion, many available formulations are unique, and practitioners should remain mindful of complying to manufacturer recommendations specific to individual brands. This is particularly relevant to the indication(s) for use, acclimatisation of the skin prior to treatment, performing the treatment and post-treatment care. Contemporaneous photographs and clinical documentation at each clinic visit, prior to and following treatment are key, particularly for courses of peels whereby the results are anticipated to be gradual and span a number of months. A detailed written medical history, including a cosmetic history of treatments, noting any allergies and careful assessment of phototype, in relation to the type of peel to be undertaken is key, as well as the requirement for any prophylactic anti-viral medication [3]. It is widely acknowledged in the literature that adjunctive home care in between each peel (if performed as a course) as well as part of long-term maintenance is preferable to achieve the best possible outcomes [8], as well as strict adherence to daily sun protection.
Superficial chemical peel ingredients
Superficial peels exert their mode of action epidermally, which can range from chemical exfoliation of the corneal layer, down to the basal layer [9]. These types of peels are a popular treatment option, as they are generally straightforward and timely to perform, and do not usually facilitate visible desquamation [10]. Ingredients within this classification are able to treat a variety of mild cosmetic concerns, such as early signs of lines and wrinkles (glogau type II), dull skin, visible pores, mild epidermal hyperpigmentation, mild acne and mild acne scarring, such as localised hyperpigmentation. Some commonly used ingredients in superficial peel formulations (either as stand-alone, or adjuvants) can include:
- Glycolic acid: This popular alpha-hydroxy-acid (AHA) reduces corneocyte cohesion at lower levels of the stratum corneum and modulates desmosomal attachments between corneocytes, which facilitates specific transient exfoliation to take place [11]. Glycolic acid not only offers effective exfoliation (relative to its pH pKa and strength), it has been shown to offer a number of anti-ageing benefits, such as increasing skin thickness, improving the quality of elastin fibres, improved density of collagen fibres, as well as increasing glycosaminoglycans to help increase firmness in the skin [12]. Glycolic acid can also act as a pigmentation inhibitor and is an effective ingredient for epidermal hyperpigmentation by decreasing melanin clumping to improve skin clarity [11]. In light of its diverse range of indications, glycolic acid is frequently used to treat photoaged skin, lines, wrinkles, as well as signs of active acne, such as seborrhoea, comedonal skins as well as papules and pustules. Glycolic acid is available as a single-ingredient peel, as well as a core ingredient in many preparations, and depending upon the formulation of the solution, may or may not require additional neutralising once the endpoint of treatment has been achieved. It is the smallest in size of all AHA molecules.
- Citric acid: This is another popular AHA ingredient derived from citrus fruits, which shares exfoliating properties similar to glycolic acid, and is an α and β hydroxy acid [13] with antioxidant and chelator properties which means it is often used to treat photoaged skins and dyschromias. In addition, citric acid helps to increase the glycosaminoglycans (GAG), improving the natural moisture reservoir in the skin [14].
- Mandelic acid: This is a lipid soluble form of an AHA derived from almonds and is commonly used for its oil control and antibacterial properties. It has a larger molecule size in comparison to glycolic acid but also functions as an effective exfoliant [15]. These characteristics support mandelic acid as an ideal choice to treat oily, acne-prone skin.
- Lactic acid: This is an AHA derived from sour milk which exerts a similar mode of action to the AHA molecules described above, specifically in relation to its exfoliation and skin strengthening properties, but is advantageous in treating areas of hyperpigmentation as it has been shown to decrease melanin synthesis by directly inhibiting the tyrosinase enzyme [15].
- Salicylic acid: This is a beta-hydroxy acid with anti-inflammatory and antimicrobial properties. It has well-documented lipophilic, keratolytic and comedolytic effects with a long-standing place in the treatment of acne, both as a single ingredient and in many peel formulations [15].
- Vitamin A compounds: These are increasing in popularity, in particular retinol owing to its multi-mechanism properties in effectively treating acne, signs of photoageing, as well as reducing matrix metalloproteinases (MMP) activity (collagenase) while increasing collagen [16]. It is increasingly used as a single ingredient peel or blended with other ingredients [17]. This ingredient continues to be explored in terms of its anti-ageing potential, and has recently been developed into a double-conjugated molecule which contains a retinoid and lactic acid. Through a double hydrolysis, the ester bonds that join the molecules are broken in the skin by naturally occurring enzymes, and subsequently, the process of breaking the double bonds gradually releases the retinoid and AHA into the skin to maximise efficiency and reduce irritation [18].
Medium and deep chemical peel ingredients
- Trichlorocetic acid (TCA) is a versatile keratolytic ingredient which coagulates and denatures proteins as it penetrates the skin [7]. It is indicated for photoaged skins of varying severity, consistent with all ingredients discussed previously. TCA is available in a number of formulations in the literature, both as a single ingredient and as an adjuvant, ranging from strengths of 10-35% [7], and thus can be considered both superficial in its mode of action at lower strengths, as well as medium depth at higher strengths. TCA is an analogue of acetic acid whereby three hydrogen atoms of three methyl groups have all been replaced by chlorine atoms [19]. TCA Strengths which are greater than 35% are utilised for focal application of individual benign pigmented lesions (lentigines) [20]. ‘Frosting’ is a traditional clinical endpoint associated with TCA which corresponds to epidermal and dermal protein denaturation; as abnormal keratinocytes are replaced by healthy cells and as skin re-epithelialises, new collagen is formed [21]. Castellana et al. describe a formulation which contains TCA 33% with hydrogen peroxide and kojic acid which does not elicit the traditional visible protein coagulation and subsequent stages of whitening to the skin, or visible desquamation [22]. Instead, the formulation is reported to stimulate fibroblast growth factors without disrupting the skin barrier, with the hydrogen peroxide facilitating the affinity of the receptor to stimulate biorevitalisation to the papillary dermis [22]. Similarly, TCA is also formulated with phenol in strengths ranging up to 30%, an increase which incrementally deepens penetration depth, improves clinical outcome, as well as increasing tolerability [23].
- Phenol shares similar protein coagulation properties to TCA but is more potent, even at lower concentrations, with the ability to elicit complete epidermolysis in keratinocytes, with melanocytes becoming partially incapacitated in the basal layer, even at lower concentrations, such as 1-4% [23]. The depth and quantity applied can significantly influence the depth [20]. At higher concentrations, as a standalone ingredient, or when blended with other ingredients, such as TCA, this ingredient is indicated to treat severe signs of photoageing in lighter skins, such as severe rhytides and advanced solar elastosis [24]. At concentrations of 15% phenol, or greater, many formulations combine the addition of croton oil which is a vegetal mix of phorbal esters. These compounds display a broad range of biologic activities over several proteins and enzymes [24]. Croton oil, a dermolytic agent, is able to facilitate an even, progressive and controlled coagulation epidermally and dermally, relative to the strength of the formulation used. At higher strengths of 15% and upwards, it can stimulate mid-reticular dermal injury with marked collagen formation and organisation of elastic fibres [25]. In addition, phenol possesses anaesthetic properties with the ability to stimulate fibroblast activity in the mid-dermis and deep dermis. At higher strengths, phenol is indicated for the face only, owing to the depth that can be achieved with a phenol / TCA blend, which can necessitate close cardiovascular monitoring during application and a rigorous post-treatment support and care pathway as occlusion during healing may be necessary.
Conclusion (and final thoughts)
The aim of this paper has been to provide an overview of some of the commonly used ingredients in chemical peel formulations. While the ingredients have been described according to depth mainly as single ingredients, many of these span formulations as blended peels, as well as adjuvants ranging from superficial to medium depth, which sit outside these traditional classifications when considered as single ingredients. It is key for clinicians to respect the differences in formulations between brands, which applies to the same ingredients in different formulations, and individual protocols for use. The continuous evolution of chemical peels offers the clinician many cost-effective and efficacious formulations to treat a variety of cosmetic skin concerns to enhance many treatment outcomes and facilitate repeat patient visits.
References
1. O’Connor AA, Lowe PM, Shumack S, Lim A. Chemical Peels: A review of current practice. Australasian Journal of Dermatology 2018;59:171-81.
2. The Aesthetic Society. Aesthetic Plastic Surgery National Databank Statistics 2019.
www.surgery.org/sites/default/
files/Aesthetic-Society_Stats2019Book
_FINAL.pdf
[Last accessed 24 June 2020].
3. Soleymani T, Lanoue J, Rahman Z. A Practical Approach to Chemical Peels: A Review of Fundamentals and Step-by-Step Algorithmic Protocol for Treatment. J Clin Aesthet Dermatol 2018;11(8):21-8.
4. Landau M. Chemical peels. Clinics in Dermatology 2008;26:200-8.
5. Fischer TC, Perosino E, Poli F, et al. Chemical peels in aesthetic dermatology: an update 2009. J Eur Acad Dermatol 2009;24:281-92.
6. Hassan KM, Benedetto AV. Facial skin rejuvenation: ablative laser resurfacing, chemical peels, or photodynamic therapy? Facts and controversies. Clin Dermatol 2013;31(6):737-40.
7. Pathak A, Mohan R, Rohrich RJ. Chemical Peels: Role of Chemical Peels in Facial Rejuvenation Today. Past Reconstr Surg 2020;145(1):58e-66e.
8. Chaudhay S, Dayal S. Efficacy of Combination of Glycolic Acid Peeling With Topical Regimen in Treatment of Melasma. J Drugs Dermatol 2013;12(10):1149-53.
9. Berson DS, Cohen JL, Rendon ML, et al. Clinical Role and Application of Superficial Chemical Peels in Today’s Practice. J Drugs Dermatol 2009;8(9):803-11.
10. Dreno B, Fischer TC, Perosino E, et al. Expert Opinion: Efficacy of superficial chemical peels in active acne management-what can we learn from the literature today? Evidence-based recommendations. Journal of the J Eur Acad Dermatol 2010;25:695-704.
11. Ditre CM, Griffin TD, Murphy GF, et al. Effects of alpha hydroxyacids on photoaged skin: aa pilot clinical, histologic and ultrastructural study. J Am Acad Dermatol 1996;34:187-95.
12. Green BA, Yu RJ, Van Scott EJ. Clinical and cosmeceutical uses of hydroxyacids. Clinics in Dermatology 2009;27:495-501.
13. Tang SC, Yang JH. Dual Effects of Alpha-Hydroxy Acids on the Skin. Molecules 2018;23(4):863.
14.Bernstein EF, Underhill CB, Lakkakorpi J, et al. Citric Acid Increases Viable Epidermal Thickness and Glycosaminoglycan Content of Sun-Damaged Skin. Dermatol Surg 1997;23(8):689-94.
15. Castillo DE, Keri JE. Chemical peels in the treatment of acne: patient selection and perspectives. Clin Cosmet Investig Dermatol 2018;11:365-72.
16. Kafi R, Kwak HSR, Schumacher WE, et al. Improvement of Naturally Aged Skin With Vitamin A (Retinol). Arch Dermatol 2007;143(5):606-12.
17. Sadick N, Edison BL, John G, et al. An Advanced, Physician-Strength Retinol Peel Improves Signs of Aging and Acne Across a Range of Skin Types Including Melasma and Skin of Color. J Drugs Dermatol 2019;18(9):918-23.
18. McDaniel DH, Mazur C, Wortzman MS, Nelson DB. Efficacy and tolerability of a double-conjugated retinoid cream vs 1.0% retinol cream or 0.025% tretinoin cream in subjects with mild to severe photoaging. J Cosmet Dermatol 2017;16:542-8.
19. Meguid AMA, Attalah DAEA, Omar H. Trichlorocetic Acid Versus Salicylic Acid in the Treatment of Acne Vulgaris in Dark-Skinned Patients. Dermatol Surg 2015;41(12):1398‑404.
20. Lee KC, Wambier CG, Soon SL, et al. Basic chemical peeling: Superficial and medium-depth peels. J Am Acad Dermatol 2019;81:313-24.
21. Chen X, Wangg S, Yang M, Li L. Chemical peels for acne vulgaris: a systematic review of randomised controlled trials. BMJ Open 2018;8:e019607.
22. Castellana R, Viana De Sa AC, Rizzi L. Fibroblast stimulation through the activation of the endocrine system for application of trichlorocetic acid. La medicina estetica 37th Year 2013;(3).
23. Deprez P. Textbook of Chemical Peels 2nd Ed. CRC Press; 2017.
24. Wambier CG, Lee KC, Soon SL, et al. Advanced chemical peels: Phenol-croton oil peel. J Am Acad Dermatol 2019;81:327-36.
25. Bertolini TM. Is the phenol-croton oil peel safe? Plast Reconstr Surg 2002;110:715-7.
Declaration of competing interests: The author is the Clinical Lead and Nurse Trainer for Aesthetic Source and KOL for Skinbetter Science and Neostrata.
![]()
COMMENTS ARE WELCOME










