Intravenous iron infusion is widely used for the treatment of iron-deficiency anaemia, especially in cases where oral supplementation is ineffective or contraindicated. Although generally well tolerated, iron infusion may be complicated by local adverse events, among which iron extravasation is particularly concerning in the aesthetic and reconstructive field, due to the risk of long-lasting pigmentary alterations and scarring.
The aesthetic impact of iron extravasation
Iron extravasation refers to the accidental leakage of iron-containing solutions from the vein into surrounding soft tissue. The complexes used in IV iron therapy, such as ferric carboxymaltose or iron isomaltoside, are hyperosmolar and may lead to significant local damage when inappropriately administered. Once in the interstitial space, iron may bind to haemosiderin and melanin, leading to persistent brownish-grey discolouration that can mimic traumatic tattooing. These skin changes may be resistant to spontaneous resolution and carry an important cosmetic burden, especially when located on visible areas like the forearm.
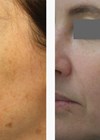
 Clinical cases before and after laser therapy – all rights reserved by the author.
Clinical cases before and after laser therapy – all rights reserved by the author.
Early recognition and multimodal treatment
Prompt identification and treatment are critical to limiting tissue damage. Initial measures include immediate cessation of the infusion, elevation of the limb, and cold compresses. Accurate documentation, including photographs and lesion mapping, is essential both for follow-up and medico-legal purposes.
For established pigmentation, treatment options fall within the scope of aesthetic medicine and dermatologic laser therapy.
Laser treatment strategies
- Q-switched Nd:YAG 1064nm laser: effective for targeting deeper dermal pigment deposits.
- Q-switched 532nm laser: more suitable for superficial epidermal pigmentation.
- Non-ablative fractional lasers: can improve skin texture and reduce the visibility of discolouration through dermal remodelling.
- Surgical excision: in selected cases where lesions are focal and cause significant aesthetic concern.
Risk factors and prevention
Recognising the causes of extravasation can help prevent occurrence:
- Technical: poor catheter placement, insecure fixation, and rapid infusion.
- Anatomical: fragile or small-calibre veins, common in elderly or chronically ill patients.
- Pharmacological: high concentration and hyperosmolarity of some iron preparations.
Strict adherence to infusion protocols, vigilant patient monitoring, and thorough staff training are essential preventative strategies.
Conclusion
While rare, iron extravasation may result in disfiguring pigmentary sequelae. In the field of aesthetic medicine and plastic surgery, a tailored, multidisciplinary approach is paramount. Laser therapies (1064nm and 532nm) offer promising results in managing cutaneous pigmentation, while surgical options remain valuable in selected patients. Prevention remains the most effective tool.
Further Reading
1. Vitale M, Zevini A, Martinelli D, et al. 532 nm Q-switched Laser Therapy for Iron Extravasation-Induced Skin Pigmentation: A Case Report and Literature Review. Cureus 2025;17(9):e92113.
2. Rampton D, Folkersen J, Fishbane S, et al. Hypersensitivity reactions to intravenous iron: guidance for risk minimization and management. Haematologica 2014;99(11):1671–6.
3. Lim HW, Collins SAB, Resneck JS Jr, et al. The burden of skin disease in the United States. J Am Acad Dermatol 2017;76(5):958–72.
4. Sontheimer RD. Iron-induced skin discoloration: a cosmetic consequence of parenteral iron therapy. J Clin Aesthet Dermatol 2010;3(10):32–4.
5. Wessels Q, Pretorius E. Skin staining caused by intravenous iron extravasation. S Afr Fam Pract 2008;50(3):62–3.
6. Dinnendahl V, Schneider LA. Persistent skin staining after intravenous iron therapy: laser therapy as a treatment option. Hautarzt 2021;72(6):495–500.
7. Cho SB, Lee SJ, Chung WS, Lee JH. Treatment of postinflammatory hyperpigmentation using Q-switched Nd:YAG laser. Dermatol Surg 2010;36(6):885–90.
Declaration of competing interests: None declared.