
The construction sequence in head and neck anatomy.
The human body is anatomically complex, and this makes the teaching of human anatomy, at the outset, a tricky exercise. Add to this the fact that there are areas where the density of structures, the multiplicity of tissues, the multiple interconnections between layers, and the small size of these entities concerned renders their appreciation, understanding, and ultimately their surgical navigation very challenging indeed.
Examples of such areas are the human hand, or the head and neck – areas requiring a detailed grasp of their three-dimensional construction if inadvertent injury to delicate and sometimes essential structures is to be avoided.
Education
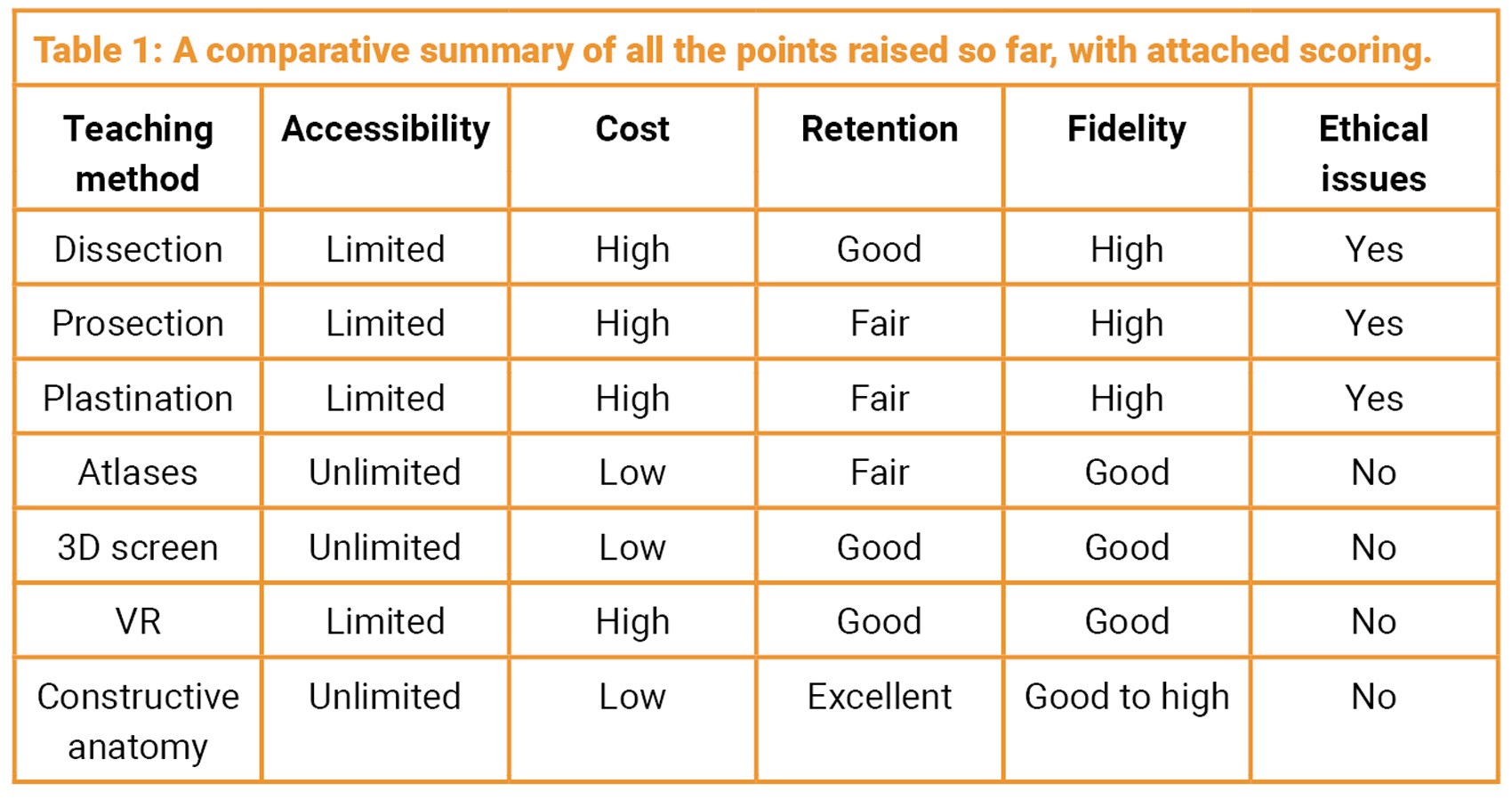
Historically, it can be said anatomical teaching has been delivered as a passive or an active exercise. Passive teaching has involved two-dimensional atlases with verbal descriptions, their digital counterparts, or the simple visual inspection of a wax model or a cadaveric prosection. On the active side of training, the rapidly advancing virtual world, with its ‘holy grail’ pursuit of true fidelity and immersion, alluringly offers a potentially viable alternative to material real-world options.
In contrast to this, cadaveric dissection has, for centuries, actively engaged anatomy students. Exploiting this real anatomy, prosection and plastination are still passive learning options, with the disadvantage of the loss of engagement in the learning process. All these cadaveric options have become hampered by the very significant expenses of wet lab staffing and maintenance, the cost of the cadavers themselves, and issues of human tissue disposal, and ethics. Thus, it is here we should introduce the most recent option of high-fidelity synthetic anatomy.
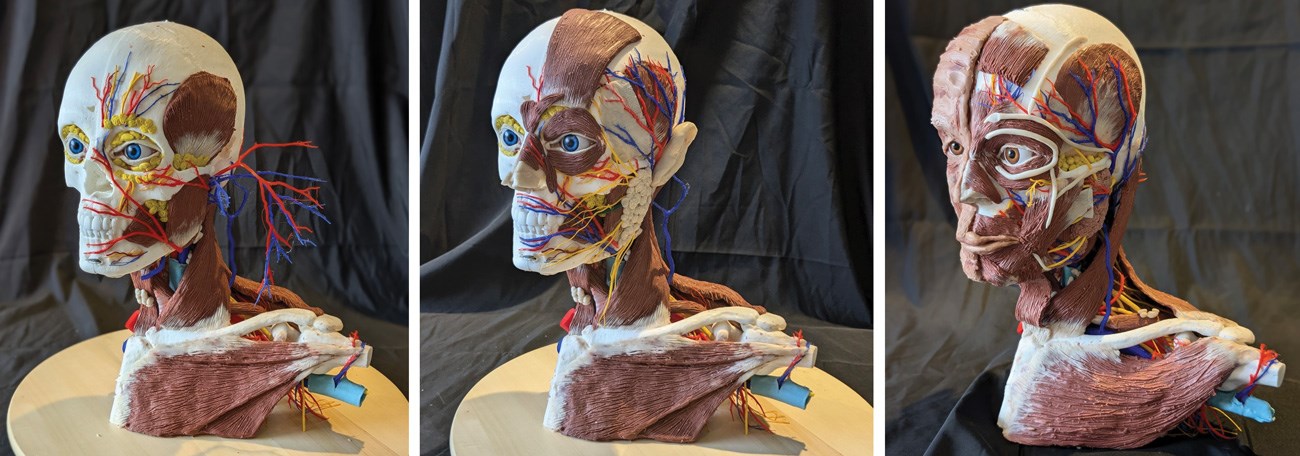
The principle in this teaching paradigm is of Constructive Anatomy™, whereby human anatomy is taught and learned by a student who will physically build their own intricate 3D anatomic model in the real world. Starting with the skeleton, they then work from deep to superficial, constructing and placing each element, muscle by muscle and nerve by nerve. This approach can be translated to all anatomy of the human body.
Modelled anatomy
Three-dimensional computer modelling and printing now allows for anatomical representation in great detail and accuracy, with synthetic filaments faithfully representing organic tissue colours, textures and pliability. Even the systematic (inside-out) modelling sequence is arguably an advantage over the disassembly (outside-in) principle of cadaveric dissection. Yes, training in surgery itself benefits by the realistic activity of dissection. But the ontogenic design of the body has fundamentally involved an inside-out vector, and assembly therefore lends itself to a profound understanding of both structural and functional principles.
Once constructed, the models allow for surgical simulation, can be kept as a reference source, and can be used for revisional reassembly. The model kits can be affordably produced, easily transported and assembled in any setting without the financial and ethical constraints that apply to human tissue options and technology-dependent training systems. And they can allow for the teaching of complex anatomy in areas of the world where such training opportunities have, for the above reasons, been limited or absent.
Our courses
Our efforts to establish anatomical assembly as a training tool has been extremely well received over a number of courses conducted over seven years, principally in hand and forearm, and head and neck anatomy. Interest in our teaching methods and programmes has been steadily increasing. This has come at a time when there has been a noted progressive decrease in the time and attention given to anatomical training in medical curriculae – at the expense of competency, let alone excellence. This diminution of anatomical training does a fundamental disservice to the communities that doctors serve. Anatomical training has, by its reliance on human material or complex computerised systems, become cumbersome and expensive. Our methodology offers a financially viable, exciting and indeed enjoyable alternative.
A curricular option?
There are a number of domains in healthcare where training with such models would be effective. In medical schools and in undergraduate training, we have had experience in using model assembly to instruct in whole body musculoskeletal anatomy, using a scaled-down full-body skeleton to engage four students (two per side) at a time.
Intermediate-grade students (the intercalated group) have had more detailed training in hand and forearm and head and neck surgery. And postgraduate specialty trainees, and indeed consultants, have engaged in these same courses that have accompanying lectures about the surgical relevance of specific anatomical parts. We would see such curricular training as a core activity, but also adjunctive to the other conventional modalities.
Physiotherapists and hand therapists have also benefitted by our courses, and there is now penetration into the cosmetic healthcare sector, supplying models for instruction in applied facial anatomy.
Summary
It would seem clear that the training paradigm presented here is more than just a viable training option, but one that carries very specific advantages over others, with few disadvantages. It warrants serious consideration for formal curricular inclusion.
Declaration of competing interests: The authors are both shareholders and directors of Surgical Sculpture Workshops Ltd, a for-profit company focused on medical education and registered in the UK.






