
Communicating information effectively with patients is essential yet often challenging. Plastic Surgeon Gavin Miller takes us through his approach to using online resources to make the process as effective as possible.
Getting ideas across to other people isn’t always easy, and with patients this can be challenging. Analogies can be helpful but often we are left with a feeling that we have failed to get our message understood. We know that patients take away too little of what is explained to them in any doctor-patient encounter. Explanatory material may have assisted, but sometimes you do not have this to hand.
The familiar expression “A picture is worth a thousand words” refers to the notion that complex ideas and concepts can be conveyed more easily with an image, or that an image of something conveys its meaning better than any description alone can achieve.
All professionals know this. Few of us would consider giving a presentation to a non-expert audience on a complex topic without the aid of explanatory pictures, videos, diagrams or graphs.
So why don’t doctors use these resources more often with their patients?
Effective communication is vital throughout the patient ‘journey’. This information exchange – a two-way process – is especially important early in the consultation process to build up rapport; this is also the time key management decisions are likely to be made. Yet, within the time constraints of a typical office consultation it can be challenging to get all the information needed from the patient, and to give patients all the information they need to make informed decisions.
Patients come to doctors for help and advice because they have a medical problem that negatively impacts on their quality-of-life, general well-being or their ability to perform day-to-day work, social or leisure activities. To help patients, doctors need to formulate a diagnosis so they can:
- Tell them what is ‘wrong’ and explain the nature of their condition
- Formulate reasonable treatment options to discuss
- Explain the effectiveness, limitations and risks of the options discussed, and select the one that best suits the patient’s needs
Medical concepts
Getting to the bottom of any patient’s problem (the ‘diagnosis’) is essentially a fact-finding exercise. The ‘data’ the doctor needs comes from the clinical presentation, the examination and special tests (i.e. investigations).
With experience this process becomes second nature to doctors. All aspects of the condition(s) they need to explain (from cause, pathology, etc. through to outcome and prognosis) is at the forefront of their minds. Yet, these are complex matters. What can be difficult for the specialist is making sure that they have effectively conveyed this multifaceted information to patients.
We know – or should know – that patients haven’t been to medical school! They often have particular difficulty in understanding anatomy and the nature of surgical interventions just from a verbal description. This is hardly surprising.
Nonetheless, doctors recognise that they must get this information across in a way that patients can understand. This information exchange also forms an essential part of the consent process before any intervention takes place:
“The seriousness and frequency of surgical risks can be conveyed in words, but explaining where structures are and what they do functionally surely requires images.”
Conveying information
Doctors have traditionally used x-rays, skeletons and leaflets when explaining clinical concepts. Nowadays, all doctors have a laptop or PC monitor on their desk, or a tablet or smartphone in their bag. So, a better and more modern way to educate patients is to use online resources; e.g. a simple internet search for images or videos (after typing in the diagnosis or procedure / intervention). Once located, these images / videos can then be used to get important points across.
I have been routinely using this in my practice for a decade or so and find it an enormously helpful and effective communication tool. Patients are grateful to me for taking the extra time involved. It also gives them confidence in you as a professional, and gives them a good impression and experience right from the outset!
Concepts that can be explained more fully using online resources include:
- Anatomy and microanatomy
- Pathomechanics
- Pathophysiology
- The nature of proposed interventions
- Potential risks and their consequences
As a hand surgeon, how better to explain to a patient what their hand condition is, how it has developed, how I propose to treat it, and what structures in the hand and fingers are at risk from iatrogenic injury when I operate on them? (Figures 1 and 2).
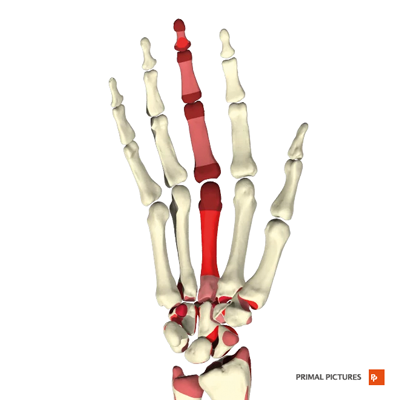
Figure 1.
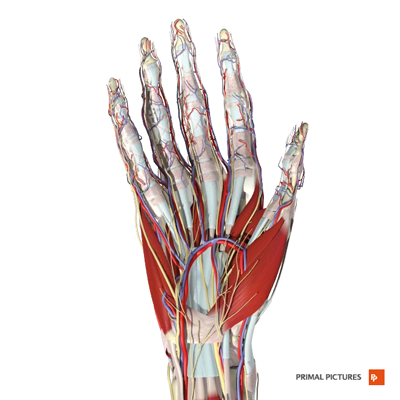
Figure 2.
In reconstructive surgery, flaps and potential donor site morbidity can be explained with images and videos rather than words. Show any patient the gracilis muscle and they will better realise: a) its utility for the proposed surgery; b) the consequences of not having it; and c) why they are likely to have numbness affecting the thigh and knee afterwards or, rarely, a painful neuroma (Figures 3 and 4).

Figure 3.
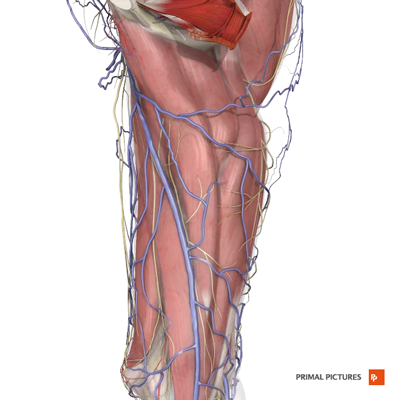
Figure 4.
In aesthetic surgery, structures to be modified – and structures at risk from injury (for example, the facial nerve during face-lifting) – can be easily appreciated by the patient (Figures 5 and 6).
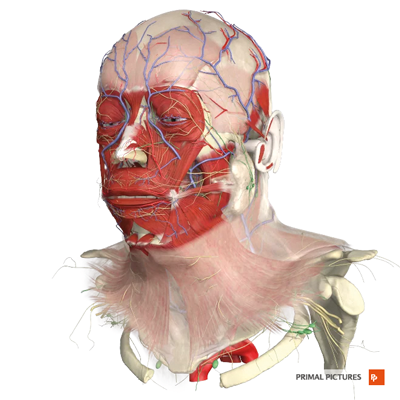
Figure 5.
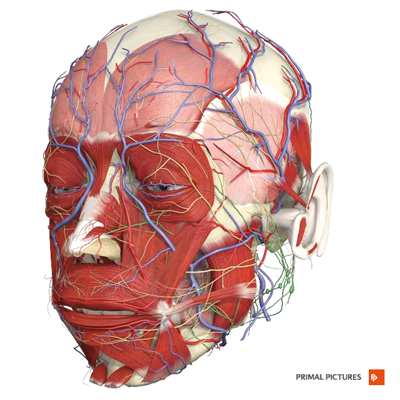
Figure 6.
The seriousness and frequency of surgical risks can be conveyed in words, but explaining where structures are and what they do functionally surely requires images. When trainee doctors and surgeons, we had the opportunity to understand difficult concepts in medicine and surgery with the help of teaching aids. Patients should have this opportunity too!
Helpful tips for colleagues:
- You’ll be doing this right in front of the patient, so it may take some practice until you become comfortable, and it becomes routine for you
- Set up your office to avoid the desk being an artificial barrier between you and the patient; if the patient is sitting at the side of the desk they should be able to see the screen or monitor if it is angled correctly – if they have any problems then get up and invite them to sit in your chair to get closer to the screen
- Be wary of showing overly gory images of surgical operations or nasty injuries – some patients don’t like (check with them first what they are happy to be shown)
- Write down the diagnosis / intervention etc. together with suggestions for helpful websites on your business card and give it to the patient with an explanatory leaflet on their condition; they can then do some ‘homework’ before they see you next
- Videos can take up more of the consultation time than simple images, so it’s normally better to direct the patient to the relevant site for review after the consultation
- Make a note in your clinic annotation that you have enhanced the consultation / consent process by using explanatory images or videos (for medicolegal reasons . . . it is a sign that you have been thorough)
While many doctors adopt a similar approach with patients, I have observed that many do not. This is surely a missed opportunity for the doctor, and the patient. As a clinician, I have found using the internet in this way extremely rewarding. I hope you do to!
Declaration of competing interests: None declared.
Acknowledgement:
Figures 1-6 are published with permission of Primal Pictures (https://primalpictures.com/).
COMMENTS ARE WELCOME



