
Dr Foutsizoglou shares his thoughts on a recent innovation based on epidermal grafting that could be used on vitiligo patients.
I attended the ‘Make Better Summit Meeting’, an international surgical congress organised by Acelity™ and chaired by Professor Dr med. Ulrich Kneser, which took place in Berlin 6-8 October 2016. Over 500 surgeons from over the world had the opportunity to share their experience in clinical surgery, learn about new products and innovations, and discuss a variety of topics, ranging from what makes a modern leader to the impact of the ageing population on healthcare and the growing challenge of infection management and prevention, or listen to inspirational talks such as Katie Piper’s personal story ‘from burns to beauty’.
Other interesting topics included wound management, regenerative medicine, disaster management such as a terrorist attack (Brussels airport bombing) or gas pipeline explosion (Kaoshiung gas explosion in Taiwan), providing clinical care in war-torn countries (Syria, Libya), delivery of remote patient care, and the World Health Organization (WHO) guidelines on surgical site infections (SSIs). What caught my attention, however, and I would like to share my thoughts about, was a recent innovation based on epidermal grafting that could be used on vitiligo patients. Some really promising results were demonstrated by several dermatologic surgeons who have used a Food and Drug Administration (FDA) approved innovative epidermal harvesting system called Cellutome™, by which epidermal grafts harvested from an unaffected donor area can be applied over depigmented skin lesions as seen in vitiligo. Interestingly, this system can be easily used by a variety of medical practitioners including cosmetic doctors and nurses.

Figure 1: Katie Piper on stage delivering a powerful message about the strength of human spirit.

Figure 2: Cellutome™ Epidermal Harvesting System (KCI, San Antonio, Texas, USA).

Figure 3: Cellutome™ Harvester applied to inner thigh.
Epidermal grafting has been used in clinical medicine and surgery as an effective autologous approach to epithelialisation of a wound. Rapid epithelialisation of a wound reduces the risk of infection by restoring the barrier function of the skin. Epidermal grafts have been successfully used over trauma wounds, surgical wounds, chronic wounds, neuropathic wounds, such as diabetic foot ulcers, and other types of ulcers such as arterial ulcers, venous ulcers and pressure ulcers. The great news is that, due to the Cellutome™ harvesting system, epidermal grafting can now be used in vitiligo patients in an office setting, without any form of local or topical anaesthesia, for re-pigmentation of the depigmented skin lesions. Studies have shown that epidermal grafts are capable of outgrowth from the graft edge, and secrete growth factors that are needed for re-epithelialisation and are also responsible for melanocyte proliferation and migration, leading to re-pigmentation of the wound [1,2].
“The epidermal grafts are ready for immediate transfer to recipient sites, with minimal donor site morbidity and minimal discomfort to the patient”
To date, the most commonly used method of epidermal harvesting consists of using syringes to raise epidermal suction blisters; however, this procedure has been described as time-consuming and painful when using larger syringes or when the floor of the blisters is touched during manual harvest. The syringe method also requires multiple sittings, and inadequate handling of the graft can lead to tearing and improper orientation, causing failure of graft take [3].
The Cellutome™ epidermal harvesting device consists of a control unit, vacuum head and harvester. The harvester is positioned on the skin surface of a selected extremity, usually the thigh, and secured with a hook and loop fastener strap; the vacuum head is then applied to the harvest site.
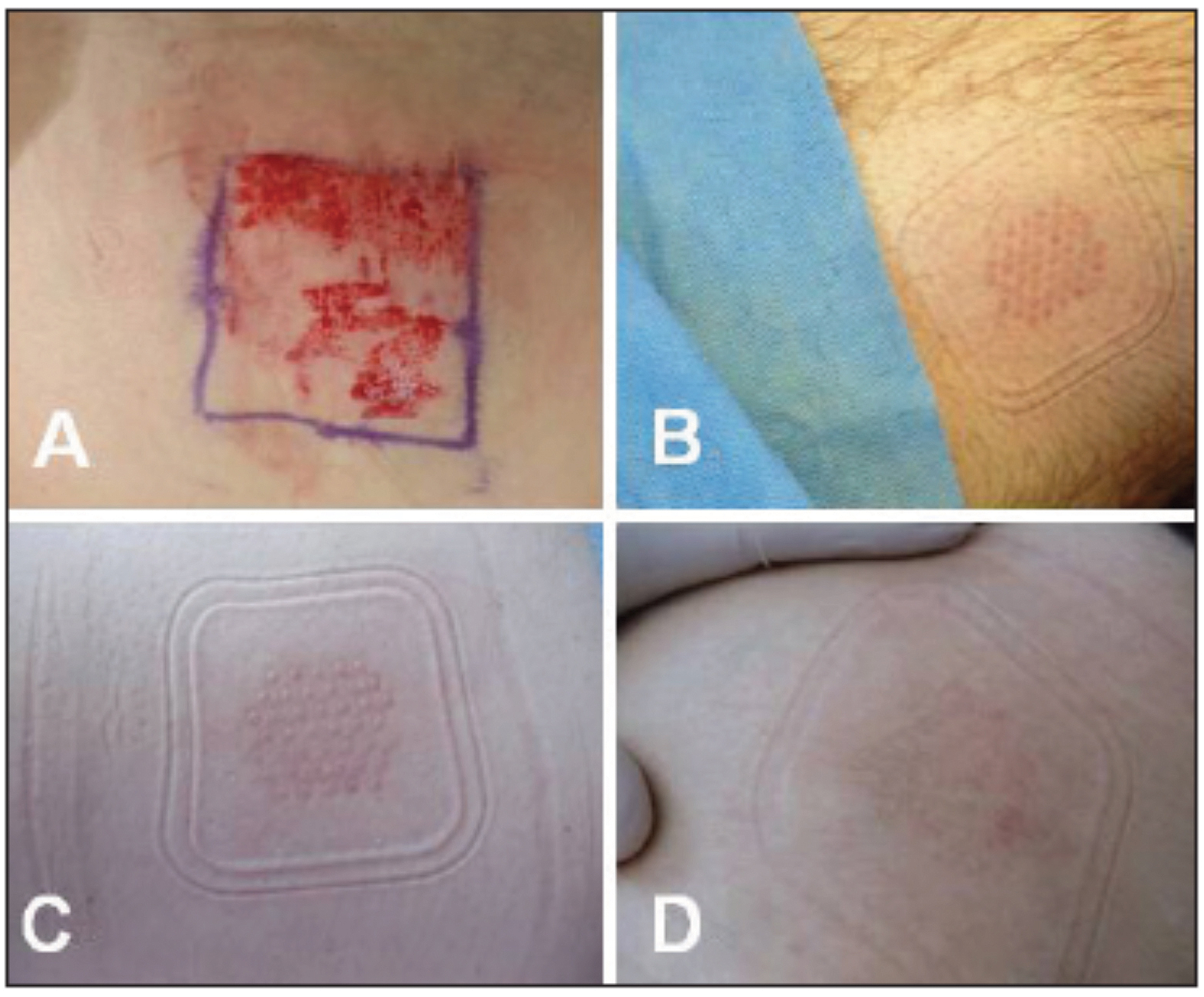
Figure 4: (A) Donor site harvested by pinch grafting; (B-D) donor sites
harvested by an automated epidermal harvesting system.
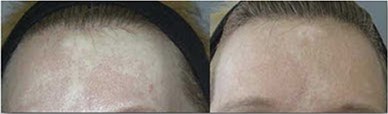

Figure 5: Before and after pics showing significant skin repigmentation, A) forehead, B) ankle,
in vitiligo sufferers using the Cellutome™ harvesting system.
This innovative epidermal harvesting system uses a combination of heat and negative pressure to create an array of 128 superficial pigment containing epidermal blisters, each around 2mm wide, producing viable and non-damaged epidermal grafts in a precise, reproducible and easy process. It then cuts the blisters in a painless fashion without bleeding because the blisters are so superficial. After microdome formation and harvesting, a standard surgical dressing is used to transfer the grafts to the recipient site. The epidermal grafts are ready for immediate transfer to recipient sites, with minimal donor site morbidity and minimal discomfort to the patient. The donor area, which is usually the thigh, heals within three or four days and the same site can be used two or three times (Figure 4). These epidermal skin grafts (ESGs) have shown in a study of healthy volunteers (n=15) to contain viable keratinocytes and melanocytes, after separation within the lamina lucida at the dermal / epidermal junction and to secrete growth factors, such as vascular endothelial growth factor (VEGF), transforming growth factor alpha (TGF-α), platelet derived growth factor (PDGF), hepatocyte growth factor (HGF) and granulocyte colony-stimulating factor (G-CSF), important for wound healing and melanogenesis [4,5]. The same study found a 99.5% average viability of epidermal micrografts created by CELLUTOME making it superior to other epidermal harvesting systems [4].
How does it work in vitiligo?
In treating vitiligo the depigmented area is abraded or lasered to create a raw surface that the dressing containing blister grafts is placed on. The dressing is clear so that the physician can see graft take and repigmentation taking place. This method has been used effectively to treat vitiligo, diabetic foot wounds, burns, pyoderma gangrenosum and traumatic wounds [6]. Most wounds heal from the edges inward, but seeding the wounds in this manner speeds up the healing process as healing occurs from the edges of the wound and the edge of each blister graft. The same principle applies to vitiligo as melanocytes from each blister graft migrate into the amelanocytic vitiligo skin lesions.
The main problems with this approach for vitiligo is some areas such as the lips, eyelids and fingers are not amenable to placement of the clear dressing and use on the neck or wrists would require the use of a cervical collar or splint in order to keep the dressing in place.
This automated and minimally invasive epidermal harvesting system produces immediate and ready-for-use autologous micrografts while causing minimal discomfort to the patient during harvesting and allowing for rapid healing of the superficial donor-site wounds without scarring. As there is currently no cure for vitiligo, this system could potentially be added into our armentarium for treating depigmented skin as it is safe, easy to use, minimally invasive and, so far, it has demonstrated some encouraging and promising results in well selected patients (e.g. small areas of depigmented skin). However, well-designed clinical trials that include representative patients of all demographics will need to be performed to confirm the effectiveness of epidermal grafting in vitiligo before any definite conclusions are drawn.
References
1. Osborne SN, Schmidt MA, Derrick K, Harper JR. Epidermal micrografts produced via an automated and minimally invasive tool from at the dermal/epidermal junction and contain proliferative cells that secrete wound healing growth factors. Adv Skin Wound Care 2015;28(9):397-405.
2. Osborne SN Schmidt MA, Harper JR. An automated and minimally invasive tool for generating viable epidermal micrografts. Adv Skin Wound Care 2016;29(2):57-64.
3. Alexis AF, Wilson DC, Todhunter JA, et al. Reassessment of the suction blister model of wound healing: introduction of a new higher pressure device. Int J Dermatol 1999;38:613-7.
4. Serena TE. Use of epidermal skin grafts in wounds: a review of an automated epidermal harvesting system. J Wound Care 2015;24(suppl 4):30-4.
5. Khunger N, Kathuria SD, Ramesh V. Tissue grafts in vitiligo surgery – past, present, and future. Indian J Dermatol 2009;54:150-8.
6. KCI data on le – Cellutome™ Suction Micrograft Harvesting System – KCI 2013.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


