
Why is rhinoplasty so important?
Facial beauty and harmony are dependent on correct aesthetic angles, volumes and proportions. The complex face is properly divided into three equal parts: forehead, nose, and lower part (where the upper lip forms a ratio 1:2 to the lower lip and chin). The noble profile forms a straight line. The nose must be straight, with an angle of 90 degrees at the tip and 110 degrees to the upper lip.
It becomes apparent, that the size and shape of the nose as a central feature is very important to the overall perception of an individual’s ‘beauty’. It can distort the straight line of the profile and break the ‘beauty triangle’ formed by the cheeks and chin.
Closed rhinoplasty
In recent years, we have seen diminishing numbers of extended traumatic operations in all surgical fields. The increasing interest toward procedures without trauma or scars, without prolonged surgery, downtime, and absence from work and social life, in both patients and doctors, has led to a notable development in minimally-invasive techniques. Rhinoplasty is no exception to this trend.
Many cosmetic problems exist, which do not need open rhinoplasty and the full armament of bone-cartilage treatment that can be more traumatic than necessary. A whole range of minimally invasive surgical and non-surgical procedures are now available for the treatment of asymmetries, smaller irregularities, post-surgical defects etc. They aim to reduce trauma and scarring, shorten or eliminate hospitalisation. They are done without general anesthesia and have shorter downtime.
These developments are reflected in the number of rhinoplasties performed globally. According to data provided by the International Society of Aesthetic Plastic Surgery we see an increase from 478,000 procedures in 2011 to 787,000 in 2016 (http://www.isaps.org/news/isaps-global-statistics).
Serdev techniques in rhinoplasty
This article provides an overview of the Serdev Techniques in rhinoplasty. These are surgical as well as suture techniques for closed rhinoplasty. The methods are minimally invasive, minimally traumatic and eliminate the need for casts or intranasal packing after surgery.
Facial analysis is critical in rhinoplasty. We do not operate on the nose as a standalone feature. The surgeon must be aware of all details of the patient’s overall appearance, the ethnic characteristics and above all – the patient’s needs and requirements. It is an artistic surgery, aiming to give aesthetic proportions and angles, as well as properly localised volumes as an aesthetic part of the whole face, which is the goal of beautification.
In specific rhinoplasty cases, Serdev Sutures® are used as separate procedures or as part of complex rhinoplasties. Their main indications are tip rotation and refinement, alar base narrowing, dorsum asymmetries and deformities, and secondary cases, where trauma is not advisable.
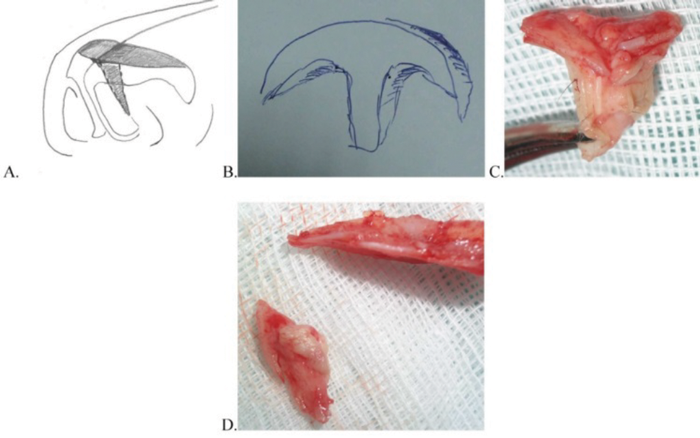
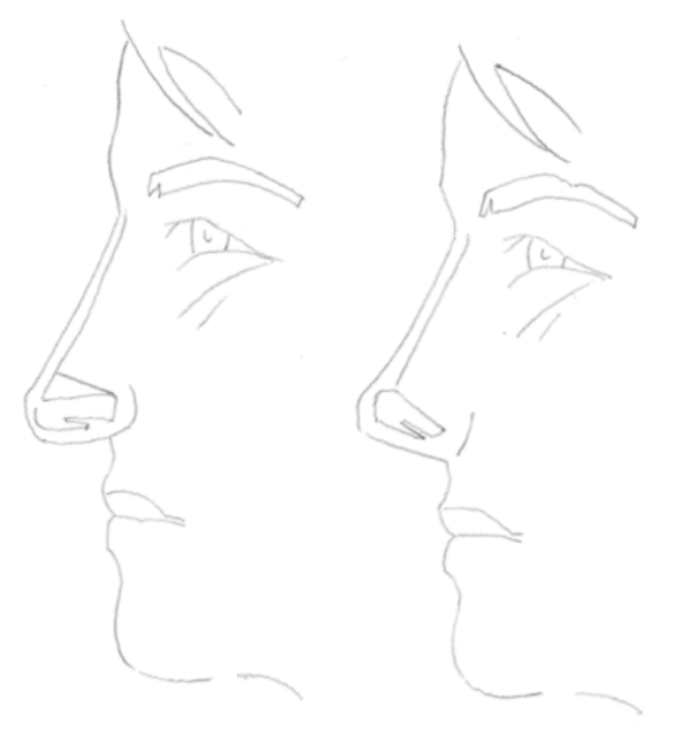
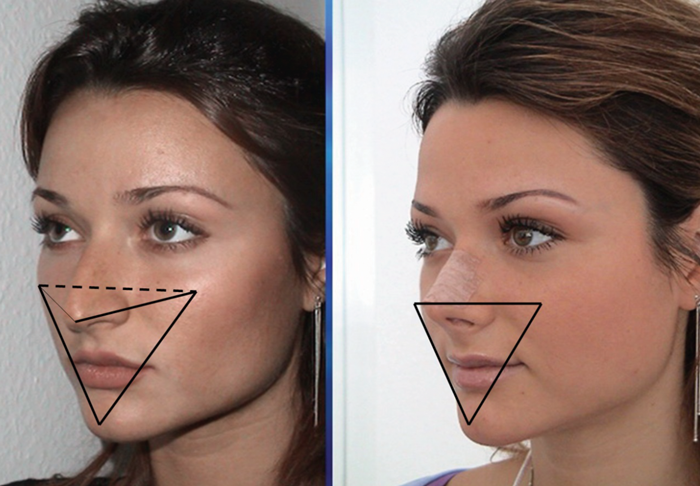
Figure 1: The T-excision en bloc for tip rotation is atraumatic, nearly bloodless and permits faster healing.
The nasal tip should be at the level of the cheekbones to make visible the beauty triangle.
Surgical techniques
T-excision for tip rotation [1]
Excision of the cephalic part of the greater alar cartilages, including unnecessary prominent caudal part of septum, permits rotation of the tip, i.e., shortening the length of the nose. It is performed to achieve upward tip rotation and involves new understanding of well-known incisions, based on anatomical knowledge and specific surgical skills. It prevents cartilages from iatrogenic trauma and devascularisation, minimises trauma, it is nearly bloodless, with no downtime for the patient, requiring no plaster, no intranasal packs, and nearly immediate return to work and social life. The T-excision technique described below is made en bloc, using a closed rhinoplasty approach and work through the contralateral nostril.
Steps:
Total retrocolumellar incision. The retrocolumellar incision will be prolonged into intercartilaginous incisions on both sides through the opposite nostril, using the opening of the retrocolumellar incision. Second septal perpendicular to dorsum incision. It will be prolonged into two intercartilaginous incisions. The T-excision en bloc is separated from the dorsal skin with a blunt tip scissor and removed. Transmucosal septocolumellar mattress suture.
T-excision could be used separately in long noses, or as a part of rhinoplasty with hump removal and other additional techniques.
Digital fracture versus lateral osteotomy [2]
The purpose of digital fracture versus lateral osteotomies is to narrow the bony base of the nose after the dorsal correction, by closing the open dorsal roof, avoiding the lateral ‘rocker’ or step-like deformities.
I apply the digital fracture technique after medial osteotomy and hump removal, in primary as well as in secondary cases. This is a simpler, safer technique, which closes the open dorsal roof after medial osteotomy much better and does not provoke bleeding and bruising. It is atraumatic and saves time during the operation and recovery. It is performed by applying lateral pressure on the nasal bone in its dorsocaudal end, using the thumb. The other hand fixes the head with opposite pressure.
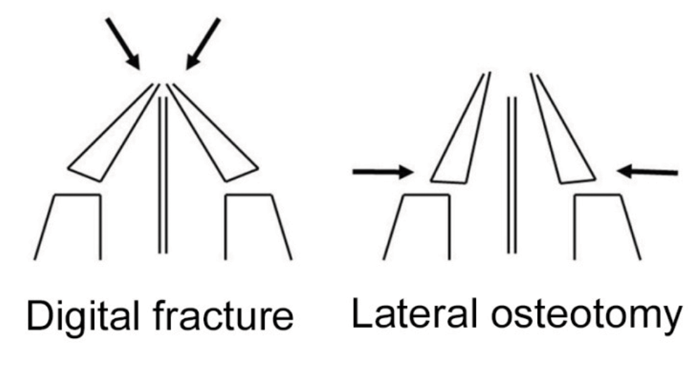
Figure 2: Digital fracture for better closing of the open roof
after medial osteotomy. It also avoids step off deformity.
Additional closed surgical techniques may be performed in more rare cases, which are not covered in this article. These are: excision of prominent posterior septal angle and nasal spine for downward tip rotation, in short upper lip or over-rotated tip; debridement of lower lateral cartilages in cleft lip-nose cases along with management of skin and fibrotic traction.
Suture techniques
NB! It is important to understand that, ‘suture’ methods are not ‘thread’ methods, regardless of the presence of threads. ‘Suture’ refers to the surgical method of suturing, i.e. bringing tissues together. It does not involve threads with hooks, barbs, cones etc.
Serdev Sutures® techniques represent scarless transcutaneous or transmucosal closed approach techniques. They could be: 1) transcutaneous methods to refine the tip or narrow the alar base; 2) transmucosal medial crura mattress sutures for tip refinement, columella sliding, and columella stabilisation; 3) refinement sutures of projected lateral crura; and 4) sutures of fibrotic tissue or upper lateral cartilages to lift depressions on the dorsum – primary or secondary.
Columella sliding for nasal tip projection using septocolumellar transmucosal mattress sutures [3]
Columella sliding is a surgical technique to correct unaesthetic / unwanted depression or projection of the nasal tip. The tip can be increased or decreased by a simple minimally-invasive technique during primary or secondary rhinoplasty as well as by a separate procedure. The main aim of the technique is to obtain the aesthetic 30° angle between dorsum and profile line.
After the T-excision in long noses or when a retrocolumellar incision is present in cases with a normal length, two to three mattress transmucosal sutures are passed from columella caudal surface to a higher point of caudal septum to give projection to the nasal tip or to a lower point to depress the tip projection when necessary.
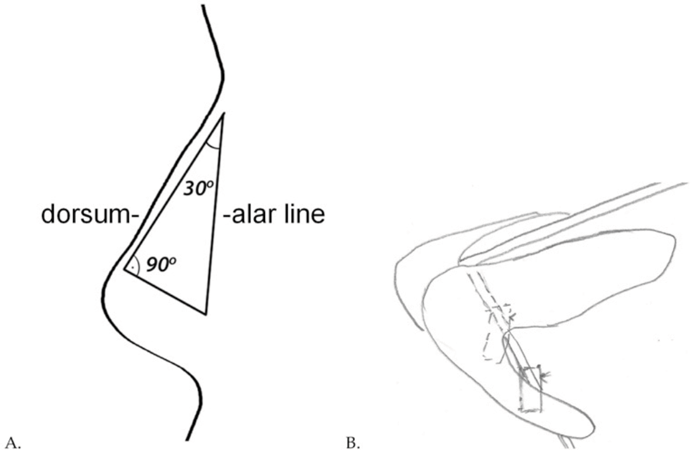
Figure 3: A. A 30 degree dorso-alar angle is responsible for best tip position and projection. B. For columella sliding, two to three mattress transmucosal sutures are passed from columella caudal surface to a higher point of caudal septum to give projection to the tip. Vice versa, the columella is sutured to lower points of the septum to lower the projection of the tip if projection is unaesthetically high.
Tip rotation and dorsum alienation [4]
Two lines of the suture are important: 1) a pass under the nasal bone periosteum, which represents the immobile subperiosteal fixation, and 2) a pass holding the mobile medial crura or all four crura of the greater alar cartilages – their suture rotation will shorten the length of the nose. Two connecting subdermal passes fulfill the circle of the suture. The suture dives without engaging skin in each skin perforation point.
In some secondary cases the suture is used to align the dorsum. Fibrosis forms the new dorsum lines during the two years before the suture will be absorbed.
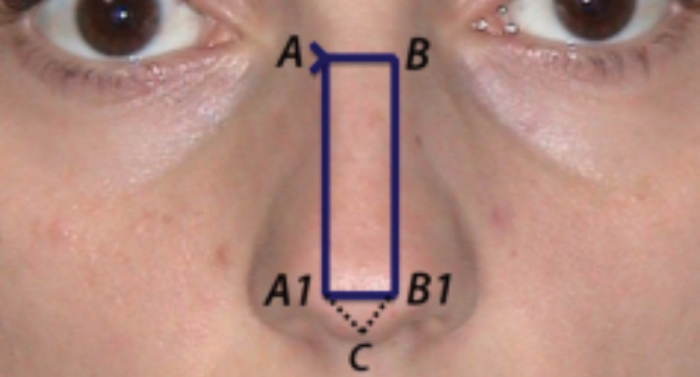
Figure 4: Tip rotation by transcutaneous suture: Pass A1-B1 holds the medial crura and rotate the greater alar cartilages and fixes them to the subperiosteal A-B pass of the suture. Pass A1-B1 can lift the drooping columella simultaneously.
Tip refinement [4]
Two lines of the suture are important: 1) a transcutaneous transdomal pass fixing the lower lateral cartilages at their most expressed convexity, and 2) a pass in the columella, holding the mobile medial crura or all four crura of the greater alar cartilages. Two connecting subdermal passes fulfill the circle of the suture. The suture dives without engaging skin in each skin puncture point. Tightening of the suture holds the domes together and refines the tip brightness.
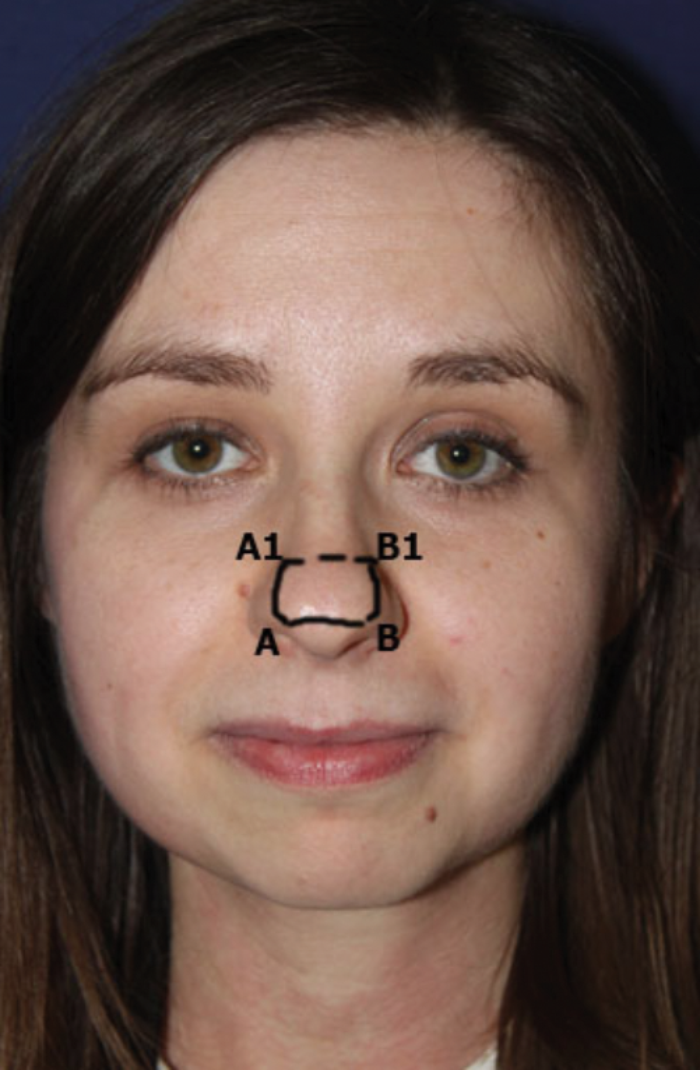

Figure 5: This transcutaneous suture represents a circle around the projected large greater alar cartilages, including both domes. It is performed using two important transcartilagenous transdomal needle passes: A-B and A1-B1 and two subdermal needle passes: A-A1 and B-B1. Pass A-B can also fix the medial crura of the greater alar cartilages to lift the drooping columella simultaneously.
Refinement of nasal medial third and / or dorsal prominence using transcutaneous suture of upper lateral cartilages [4]
Transcutaneous sutures are placed just above the nasal bones and lower lateral cartilages to fix fibrotic tissue, in order to project the soft tissue and skin. The dorsal part of cartilages could be sutured as well. A fixation of cartilages to the septum in primary and secondary open roof cases can be used for this purpose as well. In addition, these sutures narrow the nasal dorsum.

Figure 6: A secondary rhinoplasty case with T-excision, columella sliding and serial sutures along the dorsum to achieve refinement – transcutaneous sutures placed along the cartilagenous dorsum of the nose at the medial and inferior thirds, and tip of the nose to narrow the entire dorsum.
Alar base narrowing [4]
The aesthetic angle of the nostrils between the columella and lateral alae should be 30°. A wide alar base with ethnic unstable columella in Asian, Afro-American and Latin-American patients could need additional columella stabilisation suture and transdomal suture for tip refinement.
Deviations and deformities in cases of wide alar base could be different, depending on ethnicity, protruding medial crura, etc. Resection and excision techniques are well known and applicable. I often have patients coming for my suture technique, due to the fact that they reject excisions and scars.
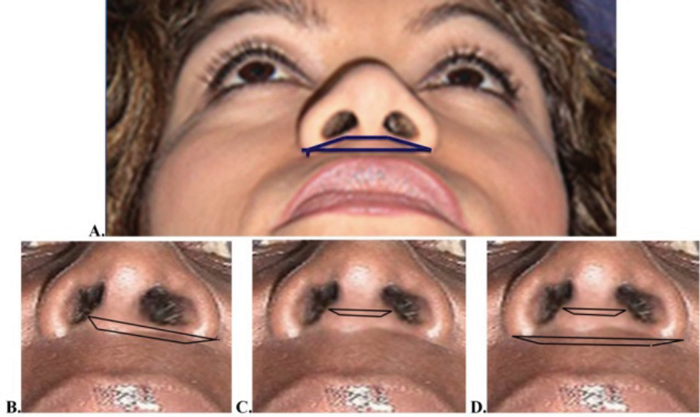

Figure 7: Alar base narrowing has the additional effect of tip projection, which
positions the flat Asian and Afro-American noses in the right profile projection.
These suture techniques can be used and repeated easily, when necessary, without downtime. The knot stays on the immobile structure (like periosteum), which provides the possibility of easily removing the suture via the same puncture points, even though this has not been necessary in my practice.
Closed rhinoplasty procedures using Serdev techniques [1-5] are easily combined with other enhancements and liftings, due to their atraumatic nature. Patients return to work and social life almost immediately. There is no bruising. Oedema is not visible for observers. Swelling can minimally change the tip position in the first five to ten days. After that it becomes natural and falls into the right position.
“Rhinoplasty, including shortening of a long nose, aims to obtain exact aesthetic proportions, volumes and angles of the face.”
Conclusion
Beautification is a work of art. Rhinoplasty, including shortening of a long nose, aims to obtain exact aesthetic proportions, volumes and angles of the face. The trend in cosmetic surgery and medicine, especially in recent years, is toward minimally invasive, atraumatic procedures. In this regard, the focus in rhinoplasty has shifted from prolonged and traumatic open procedure to a minimally invasive and atraumatic closed one.
References
1. Serdev NP: T-Excision for Nasal Tip Rotation. In: Miniinvasive Techniques in Rhinoplasty. ed. Serdev NP. InTech; 2006:3-13.
2. Serdev NP: Digital Fracture Versus Lateral Osteotomy. In: Miniinvasive Techniques in Rhinoplasty. ed. Serdev NP. InTech; 2006:29-32.
3. Serdev NP: Columella Sliding for Nasal Tip Projection Using Septocolumellar Transmucosal Mattress Sutures. In: Miniinvasive Techniques in Rhinoplasty. ed. Serdev NP. InTech; 2006:21-8.
4. Serdev NP: Transcutaneous and Transmucosal Serdev Sutures® for Nasal Tip Refinement, Alar Base Narrowing, and Other Corrections. In: Miniinvasive Techniques in Rhinoplasty. ed. Serdev NP. InTech; 2006:37-56.
5. Serdev NP: Serdev Techniques in Rhinoplasty. Voenno Izdatelstvo: Sofia, Bulgaria; 2016.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


