
What do men want when seeking facial improvement? Authors from the world-renowned European Face Centre explore the modern approach to ‘power-face’ surgery.
A growing number of men are seeking the ‘ideal face’ for physical and psycho-social reasons. Orthofacial surgery aims to achieve a balanced and harmonious soft tissue facial envelope, sound occlusion and beautiful smile aesthetics by optimising facial skeletal position.
The role of 3D soft tissue movement prediction algorithms is an integral part of osteotomy planning and preparation. This article addresses the contemporary ‘male facial ideal’, which is based on biprotrusive jaws, and a matching transverse relationship between mid and lower faces.
Background
There has been a dramatic increase in men seeking aesthetic surgery with over 1.5 million procedures performed in the USA during 2015, a significant number involving the face [1]. We have experienced a growing number of men attending for aesthetic orthofacial consultations requesting ‘stronger’ facial profiles. Hermann Sailer at the European Association for Cranio Maxillo Facial Surgery (EACMFS) conference in 2006 coined this profile ‘the power-face’ and associated this with social, sexual and professional success, whilst relieving obstructive sleep apnoea.
For over 2500 years the classical Roman and Greek facial profiles have been considered the ‘beautiful ideal’. However, applying classical canons in modern times is questionable, with a changing tide of contemporary cultural and societal preferences. A leading international fashion magazine listed all but one of their top ten male models as having relative bimaxillary protrusion and only two out of ten leading Hollywood male movie stars having the classical canon profile [2,3].
The ‘strength’ of the lower face in profile was described by Schwartz in 1958 [4]. There were three basic variations of the lower face in relation to a vertical line passing through nasion (the deepest point of the nasofrontal angle), dropped perpendicularly to Frankfort plane (Gonzalez-Ulloa 0 meridian). The profile was classified the ‘biometric average’ if the upper lip was positioned on the line. A ‘retro-profile’ was associated with the upper lip posterior to this reference and when the opposite occurred the term ‘ante-profile’ was applied. Mees et al. assessed contemporary aesthetic preferences with differing magnitudes of retroposition and anteposition of the lower face [5]. Significantly, participants of the study rated the most anterior variants of the ante-profile the most attractive profiles. This would correspond to the location of soft tissue A point 6-12mm anterior to the biometric average position in men.
In frontal view the power-face also differs from the classical and neo-classical canons. Most striking is the relationship between the four points making up the frame of the midface and lower face (zygion left and right (the ‘malars’) and gonion left and right (the ‘jaw angles’)). The classical opinion supported a tapered or trapezoid form between these landmarks. Therefore, the distance between zygion landmarks was greater than the bigonial distance. A difference of 20-30% has been considered ideal [6,7]. However, it is now accepted that in the power-face, where stronger jaw angles are favoured, a ratio closer to 1:1 is recommended [8]. This may require jaw angle augmentation alone or in combination with zygomatic ‘sandwich’ osteotomies [9]. The additional benefit of a strong jaw line in both transverse and sagittal planes is the youthful cervico-mandibular definition. Often patients with retro-profile lack jaw angle and cervical ‘step off’ definition.
“The majority of men presenting for ‘power-face makeovers’ are between 35-55 years and dissatisfied with their biometric retro-profile”
Planning
The work-up for this treatment is on a par with routine orthognathic cases. After a complete history detailing the problem and eliciting any ‘red flag’ medical and psychological conditions, stepwise anthropometric measurements are taken. Clinical photographs, articulated study models, rotational tomograph, lateral cephalogram and cone beam CT scan images are produced. For the 2D planning, the European Face Centre uses Facewizz® software (Orthoface R&D, Gent, Belgium) (Case 1 - Figure 1) to plan and simulate the desirable osteotomies [10]. During virtual planning a vertical beam parallel and anterior to the zero meridian line helps guide the virtual osteotomy segments, like runway lights, to ‘land’ in the ideal ante-profile region. Photoshop (Adobe Systems) simulations are also important aspects of the consultation for patient education and reference [11].
Three-dimensional (3D) planning is first assessed through ProPlan® (Materialise NV, Heverlee, Belgium) where the image is appropriately segmented and exported to a stereolithographic file (standard tessellation language or (stl)) that later can be used with Geomagic Sculpt software (3D Systems, Rock Hill, SC, USA), and the symmetry of the skull and the soft tissue is studied. It is important to maintain harmony with bimaxillary protrusion. Appropriate vertical facial heights and Vitruvian aspects between the lower face must be respected [12], and the effect of the advanced piriform aperture on alar base and nasal tip must be considered.
Techniques
In our practice the majority of men presenting for ‘power-face makeovers’ are between 35-55 years and dissatisfied with their biometric retro-profile. The surgical armamentarium mainly consists of bimaxillary anterior repositioning (maxilla and mandible), with or without advancement genioplasty and / or zygomatic valgisation osteotomies.
Additionally, we may have to correct narrow jaws and excess show of buccal corridors by transpalatal distraction (TPD) and / or transmandibular distraction (TMD) (Case 2 – Figures 1 and 2). If the transverse width at the gonial angles is deficient, we can also improve the proportions using particulate hydroxyapatite onlays or modifying the sagittal split osteotomy by backward rotation of the proximal segment [13].
A proportion of these patients may also elect for customised 3D printed titanium jaw angle placement and adjuvant soft tissue procedures at a second stage. The latter is often not necessary because the bimaxillary protrusion acts as a reverse face lift, eliminating jowls, perioral skin deflation and submental fullness. The computer assisted design – computer assisted manufacture (CAD-CAM) technique provides a level of surgical refinement that has not previously been guaranteed with hydroxyapatite or bone sculpting. We use Geomagic Sculpt (3D Systems, Rock Hill, SC, USA) and MakerBot® (MakerBot Industries, Brooklyn, NY, USA) equipment. Virtual prostheses are designed and templates printed in our clinic. Attention to detail is also given to screw orientation for ease of placement and anatomical ‘danger zones’ (inferior alveolar nerve). Refinements can be made on patient request before titanium printing is arranged (CADskills, Gent, Belgium).
Conclusion
The beautiful male ideal has changed over the last century reflecting the influence of Hollywood, fashion and ‘powerful’ entrepreneurs. Through orthofacial surgery, patients are achieving their physical and social desires. The overriding benefit of orthofacial surgery is the skeletal role over soft tissue draping. Cosmetic fillers, alloplastic implants and microlipofilling can be unpredictable and short-lived. Soft tissue re-draping via orthofacial surgery has proven predictable and provides long-term results.
References
1. American Society of Plastic Surgeons. 2015 Plastic Surgery Statistics. 2016.
2. Remsen N. Top 10 male models of all time. Vogue September 2004.
3. Robehmed N. World’s highest paid actors in 2015. Forbes Magazine August 2015.
4. Schwartz AM. Die Röntgenostatik. Urban & Schwarzenberg 1958.
5. Mees S, Jimenez Bellinga R, Mommaerts MY, De Pauw GA. Preferences of AP position of the straight Caucasian facial profile. J Craniomaxillofac Surg 2013;41:755-63.
6. Epker BN. Esthetic Maxillofacial Surgery. Lea & Febiger; 1994 page 80:
7. Reyneke JP. Essentials of orthognathic surgery. Quintessence Ltd; 2003: chapter 4.
8. Mommaerts MY. The ideal male jaw angle – an internet study. J Craniomaxillofac Surg 2016;44:381-91.
9. Mommaerts MY, Abeloos JVS, De Clercq CAS, Neyt LLF. The “sandwich” zygomatic osteotomy: technique, indications and clinical results. J Craniomaxillofac Surg 1995;23:12-79.
10. Mommaerts MY. The surgical art of facial makeover. Volume I. Planning and operative techniques. Chapter ‘Prediction of the facial profile’,
Orthoface R&D, Sint-Martens-Latem; 2013: 77-92.
11. Büttner M, Mommaerts MY. Photoshopping the face: simulated outcomes of orthofacial surgery. PMFA News 2014;2(2):6-10.
12. Mommaerts MY, Moerenhout BAMML. Ideal proportions in full face front view, contemporary versus antique. J Craniomaxillofac Surg 2001;39:107-10.
13. Büttner M, Mommaerts MY. Contemporary aesthetic management strategies for deficient jaw angles. PMFA News 2015;2(4):6-9.
Case 1: 57-year-old male patient requesting a power-face makeover.
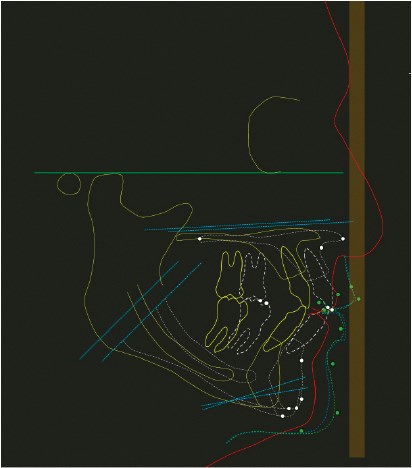
Figure 1: The recommended movements for Case 1 following Facewizz® cephalometric planning include bimaxillary advancement (9mm), sliding genioplasty (4mm), with clockwise rotation. The brown vertical beam represents the ideal ‘anteface’ zone for soft tissue A according to zero meridian of González-Ulloa.
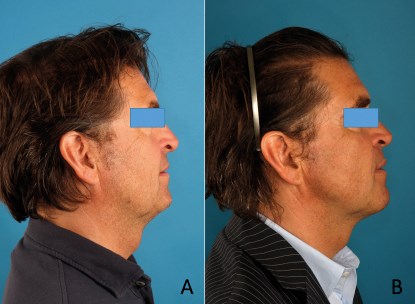
Figure 2: Preoperative (A) and postoperative (B) images of case 1. In addition to trimaxillary surgery the patient received bilateral malar valgisation osteotomies and bilateral jaw angle definition surgery with hydroxyapatite particulate. Note the skeletal advancement effect on the cervico-facial soft tissue drape. This we term a ‘reverse facelift’.

Figure 3: A. Preoperative facial oblique view; B. One-year
postoperative facial oblique view of the patient in case 1.
Case 2: 46-year-old male patient requesting a power-face makeover.

Figure 1: Preoperative and one-year postoperative images of case 2. Treatment consisted of transmandibular osteodistraction one year before trimaxillary advancement (maxillary advancement of 7mm, mandibular advancement 13mm). A strong defined jaw line and ‘Hollywood’ profile.

Figure 2: A. Preoperative full face frontal view smiling picture; B. Postoperative full face frontal view smiling picture one year later. Note improved chin dimension and improved appearance of upper incisors and buccal corridors on smiling.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME







