
This article reflects the increasing complexity of the modern world, where the rich diversity of culture, morals, the law and religion, can have profound effects on medical practice. Sometimes there is considerable debate which is not in fact appropriate. This is illustrated in the concerns about stem cell therapy and research where vocal commentators from the world of moral philosophy, the law and religion have not yet been able to distinguish between embryonic stem cell research, with the morally repugnant destruction of the fertilized embryo for the sole purpose of harnessing that life force for some other purpose, and non-embryonic stem cell research. Abortion is another contentious issue that has raised questions of morality, the law and ethics.
The extreme views can lead to extreme actions and doctors in America who perform abortions, legally, may still come under threat from those who object to the law and the action. So what about virginity? Why should female virginity be prized whereas male virginity is not an issue? What are the biological imperatives in action here? It is possible to discern public health benefits from some of the traditional religious practices (e.g. avoiding pork) but what is so crucial about proof of virginity and the sanctity of marriage? The concern extends far beyond the barriers of religion and are deeply rooted in conservative societies. A gynaecologist from North West Pakistan told me recently that even medically indicated genital surgery was considered unacceptable and some mothers would rather have their daughters die than seek lifesaving treatment.
The challenges do seem more extreme in the followers of Islam and an excellent paper has been published which discusses the issues in scholarly detail: ‘The Muslim Surgeon and Contemporary Ethical Dilemmas surrounding the restoration of Virginity’ (HAWWA 2007;5:324-9). This was written by Vardit Rispler-Chaim who is based in the Department of Arabic Language and Literature, The University of Haifa, Israel. The authors of this paper on hymenoplasty acknowledge the training they received from Dr Vishwa Prakesh who is based in New Delhi. In the next issue we will be publishing an update article from Dr Prakash where he describes his procedure for full-revirgination which is more than the simple hymenolasty. Whilst knowledge of techniques is essential it is also important to be aware of the state of the law. In this respect more guidance is needed with regard to what constitutes female genital mutilation in its broadest of definitions and reconstructive female genital surgery for ‘non-medical’ indications. We welcome comment and discussion on these sensitive but very important matters.
Prof Andrew Burd, Editor, PMFA News.
Hymenoplasty is a controversial surgical procedure that begets many ethical questions, in terms of social, cultural and medical issues. Virginity in females is a highly prized commodity in certain cultures and carries familial honour where non-virgins can face prejudice, social ostracisation and even death as they are considered to be bringing shame to the family.
The notion of a ‘one size fits all’ approach in condemning or criticising hymenoplasty as a frivolous procedure that promotes deceit and encourages female oppression fails to identify socio-cultural aspects that are prevalent in the patient group seeking hymenoplasty. This paper explores the socio-cultural and religious factors involved in women seeking hymen reconstruction and the medico-legal and ethical principles that guide surgeons in offering and performing hymenoplasty. Proper training in hymen reconstruction should be offered to plastic surgeons and gynaecologists as hymenoplasty should not be trivialised as a simple, risk-free surgery.
Background
Hymenoplasty is defined as the surgical restoration of the structural integrity of the hymen [1]. Various techniques have been described in the literature concerning hymenoplasty [1-3]. It remains a controversial procedure that raises many ethical questions [4]. The hymen is often torn during a girl’s first experience of sexual intercourse and as such can represent the ‘loss of innocence’ and a rite of passage from girl to woman. While this is acceptable to many modern societies, loss of virginity in some cultures can bring about shame, humiliation, ostracisation and possibly even violence in the form of honour killings, resulting from husbands and families discovering from blood-free sheets that their wedding night had not been the bride’s first sexual experience [5].
In social and religious cultures that stress the importance of virginity, this could mean the difference between life and death. Brides-to-be who are unable to prove their virginity when they marry have been executed in order not to tarnish family honour [6]. Reports of these type of killings have grown exponentially in secular states in the Middle East and in Iran [6] as well as in some Western countries such as France [7].
It is important to understand that cultures differ and social norms accepted by one culture or country may not be deemed acceptable to another. People tend to identify with those who hold similar values and beliefs to themselves, sometimes vilifying those who differ. This ‘us versus them’ mentality is prevalent in many socioeconomic and cultural aspects of society. In this sense, it helps to be non-judgemental and attempt to understand that empathy is crucial in dealing with this subject matter. In Iran, engaging in premarital sex is considered a crime based on the code of ‘Crimes Against Chastity and Public Morals’ based on Islamic Shariah law [8]. In totalitarian regimes or societies in which the government imposes the law based on their religious interpretation in order to guide its citizens toward a life of acceptable morality, the lines between sin and crime are blurred.
In 2008, a French Muslim couple in Lille had their marriage annulled because the wife was not a virgin. The French court upheld the annulment because the woman admitted to lying about her virginity [9]. The verdict was based on article 180, paragraph 2, of the French Civil Code, which allows for annulments based on “errors” pertaining to the “essential qualities” of the person [9]. In this case, the tribunal accepted that a woman’s virginity could be interpreted as an “essential quality” of the person [9]. While the hymen may be torn via strenuous exercise, use of tampons or as a result of a fall by women who have never had sexual intercourse, many still erroneously believe that bleeding during the first act of sexual penetration (blood on the marital sheets) is the hallmark of virginity [1].
Should surgeons offer and perform hymenoplasty? Is it ethical and legal to perform such a surgical procedure? Are surgeons helping these women deceive others? Or are they helping these women regain acceptance and integration into society? Should these ‘deflowered’ women be left to a life of social ostracisation facing prejudice and harm or should they be given a second chance in life?
Discussion
Unlike many modern women seeking hymenoplasty to surprise their partners or giving it as a gift to their husbands – the chance to make love to a virgin [10], the ethics surrounding hymenoplasty in women seeking virginity restoration for social or religious reasons are debatable. The official stance of the American College of Obstetricians and Gynecologists is to discourage the procedure of hymenoplasty, stating that the marketing of such procedures is “troubling” and that its safety and effectiveness have not been documented [11].
It is very easy to dismiss the whole notion of hymenoplasty as a frivolous procedure that is promoting a culture of hypocrisy and deceit. Acting in this manner denotes passing judgement which undermines the emotional intelligence of the medical profession as a whole. Conflict occurs in every organisation. Different beliefs and values often come into disagreement with each other. We certainly cannot believe that only one viewpoint and opinion is the right one or the ‘ultimate truth’. Such convicted beliefs have led to wars and bloodshed on a larger international context.
Beneficence and non-maleficence are two aspects of medical ethics that need to be considered [12]. Non-maleficence carries the notion for the doctor to do no harm [12]. Beneficence refers to action that will help or benefit others [12]. These two aspects taken together remind doctors to act in a manner that cultivates benefit for the patient, and simultaneously protects the patient from harm. Concepts of harm and benefit are influenced by clinical context, and thus cultural, social, religious and political factors add up to how beneficence and non-maleficence are utilised for ethical decision-making.
Doctors should first ‘do no harm’, an ironic yet altruistic piece of advice [12]. Doctors inflict harm all the time, be it from inserting a cannula or chest drain to incising an abscess or in this case performing hymenoplasty. Whilst it is often necessary for a doctor to do ‘harm’ in order to benefit the patient it is imperative that the benefits from the procedure outweigh the harm. A direct literal interpretation of ‘first do no harm’ would lead many doctors to do nothing at all in the first instance.
A woman seeking hymenoplasty is an independent agent who has the right to decide her actions in life and exert control over her own body. It is important for the surgeon to respect the patient’s beliefs even if they are in stark contrast to his or her own beliefs and / or religion. The principles of beneficence and non-maleficence are best examined in light of the principle of respect for autonomy. Surgeons run the risk of forgetting their role as healers, and appointing themselves as presiding social judges.
Some surgeons oppose hymenoplasty with the reasoning that it is deceitful and promotes an unhealthy culture of oppression of women [13]. By the same token, by denying these women access to surgical treatment, are we are also denying them their autonomy and right to live in cultures where virginity is an integral aspect for life and social acceptance? For the woman who seeks hymenoplasty, remaining in her community might also be a prerequisite for getting married and for the enjoyment of essentially life itself [14].
The Koran reiterates that a bride has to be a virgin, and according to the custom, a woman discovered on her wedding night to have been ‘touched’ brings dishonour to her family [15]. Consequences range from divorce to death [15]. To understand the problem of why some women are seen as bringing shame and dishonour when they engage in pre-marital sex, we have to also look into the cultural interpretations of the values of purity, chastity, beauty, honour and masculinity [16]. It is vital to also note that there might be social consequences for men in these cultures who are expected to prove their ‘manliness’ by marrying a virgin and deflowering them. These are all serious issues that we have to consider when a patient presents with a request for hymen reconstruction surgery. If, by denying hymenoplasty treatment, we create undesirable and harmful consequences for the patient, then we are not abiding by the principle of non-maleficence. Certainly, imposing our own concept of justice and what is socially or morally acceptable onto another culture can lead to more conflict in expense of the patient.

Figure 1: Ruptured hymen showing remnants.
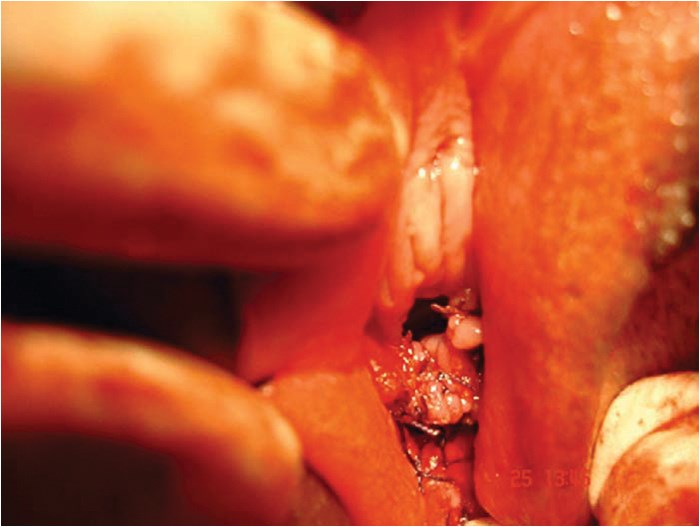
Figure 2: Completed hymenoplasty.

Figure 3: Combined hymenoplasty with labial trimming and clitoral dehooding.
In an ideal world, surgical training should be provided to gynaecologists and plastic surgeons to perform hymenoplasty safely and effectively (Figures 1-2). The hymenoplasty procedure can be combined with labial trimming (labial hypertrophy being a mark of frequent sexual intercourse), vaginal tightening and clitoral dehooding (Figure 3). Hymenoplasty should not be trivialised as a simple, risk-free procedure that can be done by any medical practitioner. Legalising hymenoplasty can also put a curb on errant practitioners performing hymenoplasty in back door clinics in unsanitary conditions. The complications such as vaginal stricture, fistulas, infection and bowel perforation that may arise from hymen reconstruction are all real and cannot be downplayed. Technical expertise and proper surgical training would be needed for a seemingly simple procedure such as hymenoplasty. Patient autonomy and confidentiality has to be strictly maintained in all instances.
Does the surgeon performing hymenoplasty show support for patriarchal norms that recommend them? Quite on the contrary, many surgeons offering hymenoplasty services are against the patriarchal norms of honour-cultures [20]. In a survey carried out, many doctors argued that surgeons or gynaecologists who perform hymenoplasties help perpetuate and support this patriarchal culture and subjugate women to male oppression [20]. On the other hand, if all surgeons and gynaecologists openly offer and perform hymenoplasties, perhaps even the most ardent patriarchs will have to accept the fact that demanding virginity is impractical in this modern era [20].
It is perhaps useful to compare performing hymenoplasty with performing a ‘bloodless’ surgery in Jehovah’s Witness patients [21]. Does performing high-risk surgery with no blood products or transfusion signify that the surgeon perpetuates and supports the beliefs of Jehovah’s Witnesses [21]? The same analogy can be applied to performing hymenoplasty [21]. Moreover, performing ‘bloodless’ surgery carries a higher risk of morbidity and mortality than hymenoplasty. So where do we draw the line? Do we subjugate every patient to our own moral and cultural perception? We have to understand the human need to belong, to be accepted and loved by their subcultural group with their own values and beliefs. We cannot attack other’s religious or cultural beliefs even if they conflict with our own and cannot violate basic human rights by withholding medical or surgical treatment.
Summary
In conclusion, the decision of whether to perform hymenoplasty needs to be reinterpreted in the context of other moral principles, such as justice and respect for autonomy. The question of whether hymenoplasty is ethical or not should not preclude women seeking the procedure gaining access to the highest quality of care. An ‘abnormality’ must not just be judged by its outer appearance or what we believe to be trivial in our own interpretation of life. The psychological and social impact has to also be considered. We as doctors and surgeons have to fight the temptation to base our medical decisions on a social paradigm of normality or projected moral superiority but to place emphasis on the patient’s wellbeing.
References
1. Prakash V. Hymenoplasty - How to do. Indian J Surg 2009;71:221-3.
2. Wei SY, et al. A new surgical technique of hymenoplasty. International Journal of Gynecology & Obstetrics 2015;130(1):14-8..
3. Ou MC, Lin CC, Pang CC, Ou D. A cercelage method for hymenoplasty. Taiwan J Obstetric Gynecol 2008;47(3):355-6.
4. Logmans A, Verhoeff A, Raap RB, et al. Should doctors reconstruct the vaginal introitus of adolescent girls to mimic the virginal state? Who wants the procedure and why. British Medical Journal 1998; 316(7129):459-60.
5. Ahmadi A. Ethical issues in hymenoplasty: views from Tehran’s physicians. J Med Ethics 2014;40:429-30.
6. Landinfo - Country of Origin Information Centre. Honour killings in Iran. 2009. http://www.unhcr.org/refworld/docid/4a704f352.html. Accessed 27 April 2015.
7. Bartels E. Maagdelijkheid en maagdenvliesherstel tussen ethiek en beleid: een reactie [Virginity and hymen construction between ethics and policy: a reaction]. Migrantenstudies 2000;16:45-53.
8. Mir-Hosseini Z, Hamzic V. Control and Sexuality: The Revival of Zina Laws in Muslim Contexts. London, UK; Women Living Under Muslim Laws; 2010. 9. Félix Rome. La mariée avait un vice caché [The Bride Had a Hidden Defect]. Recueil Dalloz 2008;184(22):1490.
10. Sciolino E, Mekhennet S. In Europe, debate over Islam and virginity. New York Times 11 June 2008.
http://www.nytimes.com/2008/06/
11/world/europe/11virgin.html?pagewanted=all.
Accessed 27 April 2015.
11. Committee on Gynecologic Practice, American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 378: Vaginal “rejuvenation” and cosmetic vaginal procedures. Obstet Gynecol 2007;110:737-8.
12. Gillon R. Philosophical medical ethics. Chichester, UK; John Wiley & Sons; 1985: chapter 13.
13. Earp BD. Hymen ‘restoration’ in cultures of oppression: How can physicians promote individual patient welfare without becoming complicit in the perpetuation of social norms? Journal of Medical Ethics 2013;40(6):431.
14. Juth N, Hansson SO, Tännsjö T, Lynøe N. Honour-related threats and human rights: a qualitative of study Swedish healthcare providers’ attitudes towards young women requesting virginity certificates or hymen reconstruction. Eur J Contracep Repr 2013; 18:451-9.
15. Kandela P. Egypt’s trade in hymen repair. Lancet 1996;347(9015):1615.
16. Tännsjö T. Hedersmoral – ett problem i västerländsk sjukvård? [Honour morality - a problem in Western healthcare?]. Tidskrift för politisk filosofi 2011;1:6-26.
17. Farshidi N. Virginity still a commodity in Iran.
http://iwpr.net/report-news/
virginity-still-commodity-iran.
Accessed 27 April 2015.
18. Sabuni N, Heimer G. Läkare ska inte göra “oskuldsoperationer” [Physicians should not perform “virginity operations”]. Svenska Dagbladet/Brännpunkt 2011.
19. Nationellt Centrum för Kvinnofrid [National Centre for Knowledge on Men’s Violence Against Women]. Att möta patienter som söker för oro kring oskuld och heder [To encounter patients with concerns regarding virginity and honour]. Uppsala, Sweden; 2011.
http://kunskapsbanken.nck.uu.se/
nckkb/nck/publik/fil/visa/296/NCK-rapport_2011-2
_Att_mota_patienter_www.pdf.
[accessed 27 April 2015].
20. Lynøe N, Juth N. Zero tolerance against patriarchal norms? A cross-sectional study of Swedish healthcare staffs’ restrictive attitudes towards young females who request virginity certificates or hymen restoration. J Med Ethics 2015;41(3):215-9.
21. Juth N, Lynøe N. Are there morally relevant differences between hymen restoration and bloodless treatment for Jehovah’s Witnesses? BMC Medical Ethics 2014;15:89.
Declaration of competing interests: Both author are plastic surgeons who performs hymen reconstruction. The lead author LS Khoo was trained in hymenoplasty under plastic surgeon Dr Vishwa Prakash of Safdarjung, New Delhi
Acknowledgement:
The authors would like to thank Dr Vishwa Prakash of Safdarjung, New Delhi for supplying his pictures (Figures 1-2) for use in this publication.
An invited commentary from Dr Refaat Karim, Plastic Surgeon,
Amsterdam, the Netherlands.
This is a complicated issue.
Three of the world’s major religions, Judaism, Christianity and Islam, all worship the God of Abraham, and therefore share some common beliefs. In all three religions sexual purity is highly valued. To insure ‘God’s law’ stoning was advocated if virginity was lost before marriage (Deut 22:13-21). (Editor’s note: I have included the full text for information as the key to the ‘virginity test’ appears to be post-coital bleeding on the bed linen. Nothing more, nothing less.)
If a man takes a wife and, after sleeping with her, dislikes her and slanders her and gives her a bad name, saying, ‘I married this woman, but when I approached her, I did not find proof of her virginity,’ then the young woman’s father and mother shall bring to the town elders at the gate proof that she was a virgin. Her father will say to the elders, ‘I gave my daughter in marriage to this man, but he dislikes her. Now he has slandered her and said, ‘I did not find your daughter to be a virgin.’ But here is the proof of my daughter’s virginity.” Then her parents shall display the cloth before the elders of the town, and the elders shall take the man and punish him. They shall fine him a hundred shekels of silver and give them to the young woman’s father, because this man has given an Israelite virgin a bad name. She shall continue to be his wife; he must not divorce her as long as he lives.
If, however, the charge is true and no proof of the young woman’s virginity can be found, she shall be brought to the door of her father’s house and there the men of her town shall stone her to death. She has done an outrageous thing in Israel by being promiscuous while still in her father’s house. You must purge the evil from among you.
A lot has changed over the last 3000 years, but virginity can still sometimes be an issue of life or death. Although it is disturbing, we cannot ignore this fact. In our shared western views, we agree that every person has a right to personal and physical integrity. Everyone has the right to personal autonomy and self-determination even of their own body. A concept which differs from the beliefs found in the holy books.
The young women who seek hymenoplasty are the product of our time and are in cultural transition. They do not believe in their old traditions, but understand that we live in an imperfect world where diplomacy and tolerance are needed. They are bridging the gap between generations and cultures and in so doing slowly changing values and are seeking a way to balance the past and the future. The authors of this article have a very important message regarding the need and indication of hymenoplasty.
An invited commentary from Professor Sanjukta Bhattacharya, Department of International Relations, Jadavpur University, Kolkata, India.
If socio-cultural morality became the prime mover of medical research (and practice), we would still be in the age of the Old Testament. Medical scientists have stretched the boundaries of existing location-based and time-bound moralities to conquer diseases and get to modern times. Medieval Christian morality forbade cadaver dissection. If this had not been done, defying the then existing social and religious norms, the various systems that help to run the human body would never have been uncovered, and science-based diagnosis and treatment would never have advanced.
Should medical practice be based on ‘socio-cultural morality’? The counter-question is which socio-cultural morality? Society is not unitary and neither is culture. There is so much overlap of heterogeneity, that many different cultures – ethnic, racial, religious, even national – can be found to co-exist within a few square miles of the same city in modern times; take, for example, New Delhi, New York or Amsterdam – all are culturally heterogeneous, where the ultra-modern co-exists with the extreme-conservative. Further, what is taboo in one country may be permitted in another. Abortion, for instance, is forbidden in Catholic, Muslim and many other cultures, but in India, which is predominantly Hindu, and Hinduism is generally considered to be on the conservative side so far as cultures go (not its religious philosophy, which is just that – a mix of very divergent philosophies leaving no place for dogmatism), Medical Termination of Pregnancy (MTP) is legal and permissible up to a specified number of months (after which it may be unsafe). Confidentiality is maintained and women can use their own agency if they have reached a specified age. On the other hand, in the United States, the home of feminism, ‘choice’ was (and is) such an important issue; the Equal Rights Amendment has made headlines over several years, and there is still a big anti-abortion lobby, which feeds into and restricts research on potentially life-saving areas of medical science, for instance, stem cells. ‘Socio-cultural morality’, under the circumstances, cannot be, and is not, monolithic.
The issue also concerns women’s empowerment. While the males of certain communities may look askance at the very idea of, let alone the practice of hymenoplasty, will it not give women agency and some amount of control over their lives in those same communities? Is it ethical to let a woman be divorced or become the victim of honour killing and unethical to allow the root cause for such actions to be avoided by repairing the hymen? If honour killing is deplored, measures that may prevent it should be endorsed. Further, the very idea of shaming a woman because her hymen is torn is repugnant; the same sanctity has never been given to male virginity. It is a changing world but it is still a patriarchal world. One cannot change society overnight, though changes in attitude are happening all over the world. But as long as there are remnants of archaic / anachronistic ideas concerning women’s chastity prevalent in certain societies, cultures and classes, something should be done so that women do not become the victims of these ideas. In any case, in the modern world where exercise and sports are part of a girl’s school days (and there is no country which totally forbids girls to go to school anymore although there may be restrictions on the extent of schooling), the hymen may be torn as a result of any number of reasons. She should not suffer for men’s suspicions and limited knowledge about these things.
Further, where is the deceit in this kind of surgery? If hymenoplasty is seen as deceiving the community’s males, actors and actresses who undergo major plastic surgery on their faces and bodies, and dental surgery to have wonderful teeth on-screen, should be seen as deceiving the world, because they are not what they were.
And finally, medical ethics is shaped by the two words – beneficence and non-malfeasance (try to do good but first, do no harm). The clinical practice of hymenoplasty will benefit women who need it. The question is who will it hurt? Is it non-malfeasant? I think it is.
COMMENTS ARE WELCOME




