
This article has been verified for CPD. Click the button below to answer a few
short questions and download a form to be included in your CPD folder.

The shape and volume of the lips are highly significant features when defining ‘facial attractiveness’ in both females and male. With advancing age, the upper cutaneous lip elongates leading to increased vertical dimensions of the cutaneous portion of the upper lip, blunting of the philtral columns, inversion of the lip vermillion and reduced incisal tooth show at rest.
Additionally, loss of dentition and atrophy of the underlying orbicularis oris muscle and underlying skeletal framework will further contribute to loss of the upper lip profile curvature.
On the contrary, a ‘youthful’ lip is usually shorter, plump and curvaceous with several millimetres (ideally 2-3mm) of central incisor show at rest deemed a highly feminising trait. The upper lip lift procedure aims to rejuvenate the lower facial thirds by improving lip and smile aesthetics. This is achieved by reducing the height of the cutaneous portion of the upper lip and everting the vermillion thereby increasing incisal show.
Given the increased visibility of facial plastic surgery procedures via the internet and social media portals such as Instagram and TikTok, I am now seeing a greater number of patients who are opting for lip lift as their favoured aesthetic procedure. Patient selection is crucial for optimal aesthetic outcomes after undergoing the lip lift procedure. In my current clinical practice, there are three main indications for performing lip lift which include:
- Facial ageing due to elongation of the cutaneous portion of the cutaneous portion of the upper lip
- Facial feminisation for transgender and gender diverse (TGD) patients
- Secondary / revision cases due to inadequate shortening or excessive scar.
Lip lift procedure
As part of pre-surgical work-up, it is imperative to have good quality medical photos of the lips at rest and in animation. Generally, the lip is considered elongated when the distance is >15mm, as measured from the base of the nose to the superior part of the vermillion.
The lip lift procedure can be performed alone under local anaesthetic or in combination with other facial plastic surgery procedures under general anaesthesia. Before any local anaesthetic is administered, the exact amount of excessive upper lip skin is identified with a marking pen just beneath the nose with the patient sitting upright for absolute precision. The amount of excess skin that needs to be excised is determined by pushing the lip upwards until the desired amount of central incisor show is achieved. The preoperative markings are positioned so that a precise geometric incision tapers out towards the lateral aspects of the nose (Figure 1).
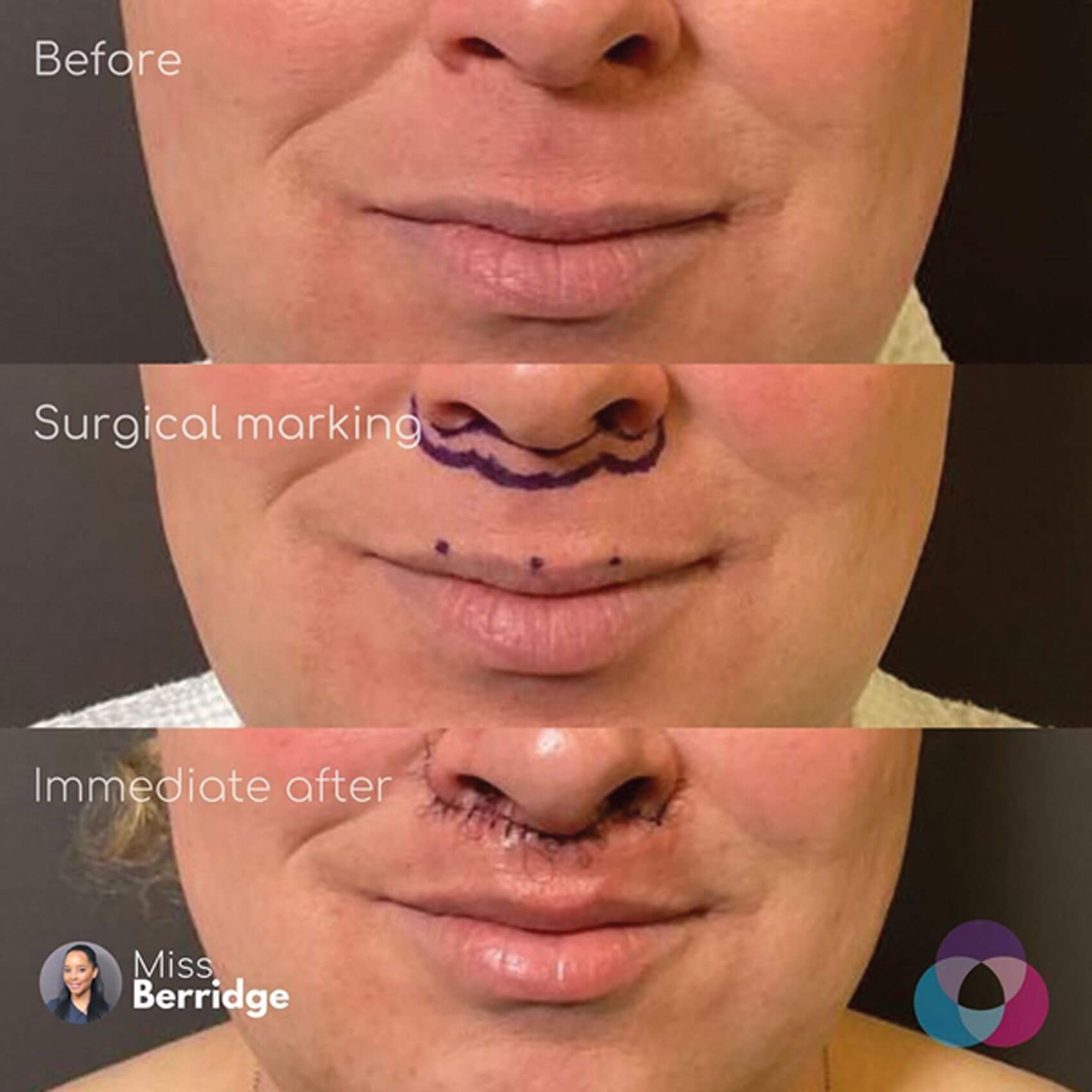
Figure 1: This image shows the patient before and after lip lift with an emphasis
on the ‘bullhorn’ pattern of excision to enable full thickness skin removal.
When using local anaesthesia, I inject enough 2% Lignospan with 1/80,000 adrenaline to optimise patient comfort but not excessively distort the tissues. Next, the skin is prepped with a non-alcoholic solution such as aqueous Chlorhexidine, being diligent not to wipe off the surgical markings. I then begin the incision with a no.15 scalpel superiorly at the alar crease, nasal sill, subcolumellar region and continue to the opposing side. Once the superior incision is complete, I then incise the inferior marking to complete a ‘subnasale bullhorn’ shaped incision. A full thickness skin-only incision is dissected leaving the underlying orbicularis muscle intact, with an appropriate amount of undermining of the caudal cutaneous lip skin to allow superior repositioning of the tissues and tension free closure (Figure 2).

Figure 2: This image shows before and six weeks after lip lift surgery, demonstrating the position of the scar.
In addition to the everted shorter lip, this image also highlights the increased incisor show at rest.
The key to skin-only resection is to ensure that the deep sutures are not fixated to the subcutaneous nasal skin but to the deeper structures around the anterior nasal spine and piriform aperture. I perform deep closure with interrupted 5.0 PDS and use 6.0 Ethilon for superficial skin closure. Alternatively sutures of the surgeon’s choice may be used. The surgical wound is dressed lightly with a coating of Tinc Benz (Benzoin Compound Tincture BP) and brown Micropore surgical tape to support the lip during the immediate postoperative period.
Postoperative care
Patients are asked to refrain from excessive animation / lip movement for the first 7 to 10 days and are asked to follow a soft diet. Sutures are removed in clinic at six days and patients are reassured about the ensuing postoperative swelling which usually settles within 10 days but can take longer. Likewise, the scar is visibly red once sutures have been removed but fades to an imperceptible scar as time progresses (Figure 3).

Figure 3: This image profiles the lateral view before and after lip lift surgery. It nicely demonstrates
the everted shortened lip, increased incisal show and fading of the scar as time progresses.
Aesthetic outcomes
Patients report a high rate of satisfaction following the lip lift procedure. Complication rates are low if due diligence is taken with both careful patient selection and surgical technique. Lip shortening surgery improves dento-facial aesthetics and is a powerful tool for any facial plastic surgeon rejuvenating the ageing face.
Further reading
1. Talei B. The modified upper lip lift. Facial Plast Surg Clin N Am 2019;27(3):385-98.
2. Pacifico M. Approaches to lip augmentation: surgical lip lift. The PMFA Journal 2018;6(1):32.
3. Gatti JE. Lip-shortening surgery. Plast Reconstr Surg 2023;152:765.
Declaration of competing interest: None declared.
COMMENTS ARE WELCOME





