
In October 2013, a female patient presented for an initial consultation. She had a past medical history of left lower seventh (facial) nerve palsy following excision of left benign parotid adenoma in 2002. This had been treated over the years, firstly with a left lower facial nerve graft in 2003 in London, and followed at a later date by endoscopic brow lift using an endotine implant. Unfortunately this did not make much difference. Nerve conduction tests showed no response from the left facial nerve, which was therefore considered completely paralysed.
She was extremely traumatised by her previous repetitive surgery and had been recommended to see me for a non-surgical option. I advised her to have a couple of sessions with Sculptra® to help volumise the left side of her face – which was showing evidence of muscle and fat atrophy due to disuse – followed by non-surgical left mid and lower facial lift with Silhouette Soft®.
I advised that Sculptra would help stimulate collagen in her left cheek area and this would help anchor the threads and therefore make the Silhouette Soft more successful in lifting her left lower face.
She also had evidence of left brow ptosis, left upper and lower lid retraction, giving her lagophthalmos (poor lid closure). In addition, the patient was keen on Silhouette Soft for a left brow lift but I did not feel this would give her a long-term solution and also would pose a further risk of corneal exposure and ulceration because of her lagophthalmos. I advised her that a direct brow lift was a more permanent option in addition to a platinum weight for her left upper lid.
Method and results
One vial of Sculptra was injected into the patient’s left temple and midface on 7 November 2013 and a second vial was injected into her mid face and lower face on 5 December. On 9 January 2014 she had four 16 cone Silhouette Soft threads inserted into her left mid and lower face (each thread has 16 cones attached to it that help anchor the threads in the subdermal plane).
There were four exit points marked, the first point was 1cm lateral to the upper half of the nasolabial fold, the second point was 1cm lateral to the middle half of her nasolabial fold, the third and fourth points were 1.5cm apart in the line between the corner of the mouth and the angle of the mandible.
This was tolerated very well and there were no postoperative problems.
I saw her for review three months later in April, and she was extremely pleased with the results – her left side had lifted and looked significantly better. The corner of her left lower lip was still downturned slightly and I therefore suggested that she had some Juvederm® ULTRA 4 placed into her marionette lines, left side more than right to help improve this further. I also gave her four units of Botox into her left levator anguli oris muscle to complement the filler treatment.
Since then she has also undergone left direct browlift in addition to upper lid blepharoplasty under local anaesthetic on 10 May 2014. A platinum weight for the left eyelid was not deemed necessary as there was adequate eye closure and she had a good Bell’s phenomenon. Nine days later, her left eyebrow position was very good and her sutures were removed, she had made an excellent recovery and was very pleased with the outcome. Her last check up was in June 2014 and her left brow position and left mid face and lower face are well maintained with adequate lift.
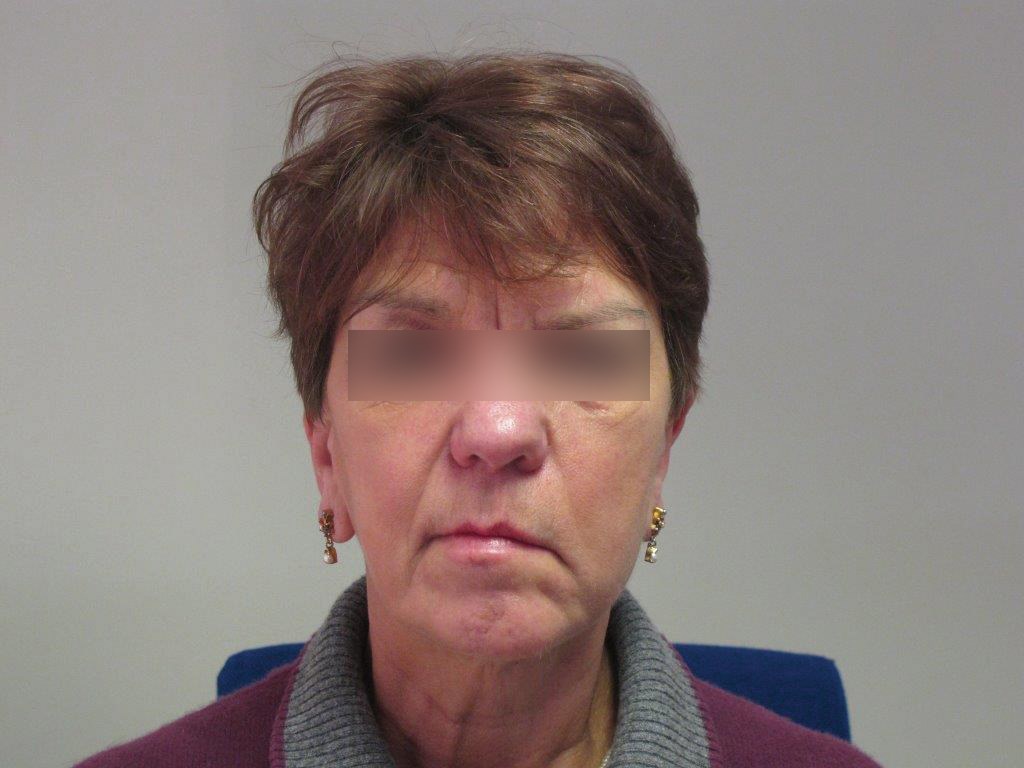
Figure 1: Before treatment.

Figure 2: Following treatment with Silhouette Soft.
Discussion
Facial nerve palsy is a feared complication of head and neck surgery and cancer. There are huge psychosocial and functional implications for the patient. Traditional options have included gold / platinum weights inserted into the upper eyelids, tarsorraphy, microvascular free tissue transfer, interposition grafts of the facial nerve and hypoglossal facial nerve anastomosis. In patients who have already undergone significant surgery and have a complex surgical history already, further radical surgery in the form of free flaps or nerve anastomosis are often not warranted. Previous literature search shows that the Silhouette lift is an alternative solution to this difficult and often devastating condition, but so far there has not been any mention in the literature of using Silhouette Soft for this.
In the literature, facial rejuvenation and improvement of malar projection / jaw definition using non absorbable 3/0 polypropylene sutures with absorbable cones made of L-lactic acid and glycolide polymer has been published (Silhouette lift). The Silhouette lift has been used as a mid face and lower face lifting technique in suitable patients for both cosmetic reasons and for facial palsy patients.
The Silhouette lift is a surgical procedure whereby a surgical incision is made both at the entry and exit points where the suture is inserted and removed, necessitating sutures for closure. The entry point is a 2.5-3cm incision in the temporal hairline and there are usually four exit incisions placed between the mid half of the nasolabial fold to the jawline. The Silhouette Soft technique that was used in this case, however, is entirely non-surgical, requiring only needle entry and exit points and therefore no sutures are required. This is a straightforward technique done as an outpatient in a clinic setting.
The Silhouette Soft thread and cones are made entirely from poly-L-lactic acid which are entirely absorbable, leaving behind fibrotic tissue as it dissolves to help maintain the desired lift over a 12-18 month period and is easily repeatable.
Summary
My case report is the first non-surgical option presented in the literature, using a combination of Silhouette Soft and Sculptra for lower seventh (facial) nerve palsy. This should be considered for appropriate patients who want a non-surgical and straightforward procedure which takes approximately 45 minutes to do. Postoperative complications are minimal in the form of bruising and swelling which is transient and settles within three to five days and antibiotic cream is used for three days over the entry and exit points.
References
1. de Benito J, Pizzamiglio R, Theodorou D, Arvas L. Facial rejuvenation and improvement of malar projection using sutures with absorbable cones: surgical technique and case series. Aesthetic and Plastic surgery 2011;35(2):248-53.
2. Bisaccia E, Kadry R, Saap L, et al. Novel specialised suture and inserting device for the resuspension of ptotic facial tissues, early results. Journal of Dermatological Surgery 2009;35(4):645-50.
3. Isse N. Silhouette sutures for treatment of facial ageing: facial rejuvenation, remodelling and facial tissue support. Clin Plastic Surg 2008;35(4):481-6.
4. Maschio F, Lazzaro L, Pizzamiglio R, et al. Suspension sutures in facial reconstruction: surgical techniques and medium term outcomes. The Journal of Cranio Facial Surgery 2013;24(1):e31-3.
5. Gamboa GM, Vasconez LO. Suture suspension technique for mid face and neck rejuvenation. The Annals of Plastic Surgery 2009:62(5);478-81.
6. Stephens J, De Zoysa N, Hughes J, Mochloulis G. Silhouette lift for facial reanimation. Clinical Otolaryngology, 2009;34:390-408.
7. Navarrete M, Knäpper J, Boemo R, Torrent L. Facial Asymmetry correction in Facial Palsy patients with Silhouette Sutures. International Journal of Clinical Medicine 2012;3:55-9.
Declaration of competing interests: None declared.
Editor’s comment: We welcome reports of new devices and new strategies of using products and devices that already have an established place in the market. It is customary in the scientific literature to demand at least a minimum of one year of follow-up before reporting ‘new’ procedures. As a magazine, we do not need to be so restrictive and, as stated previously, our policy is to be a platform for dissemination of information whilst making clear that publication does not automatically imply endorsement. A case report can be categorised as a preliminary report when the follow-up is less than six months and a definitive report when there has been more than one year of follow-up. We would welcome a further report from the authors later in the year to give more follow-up on this patient. This will also provide an opportunity for some constructive reflective comment which will certainly add value to the shared experience.
COMMENTS ARE WELCOME



