
‘Science’ is having a real bashing these days. Unfortunately, those who talk up ‘science’ and ‘scientific evidence’ the most are those who least understand what science is about. The Oxford English Dictionary offers the following definition: “the intellectual and practical activity encompassing the systematic study of the structure and behaviour of the physical and natural world through observation and experiment”.
Wikipedia offers up this: “Science is a systematic enterprise that builds and organizes knowledge in the form of testable explanations and predictions about the universe”.
Civilisation may die waiting for science to provide answers to all our problems. There are qualities associated with science. What we regard as the best science requires data; data that is validated and the analysis peer reviewed. The only validated data is data that reflects what has happened. Science fact, the past; science fiction, the future. As a burns surgeon I knew that too often we did not have the evidence to prove a new method of treatment would work but we did have the evidence that conventional treatments did not work. This is the push of science, the pull of science is firmly rooted in serendipity and dare I say it, luck. How many times do we hear of a scientific breakthrough that is looking for a clinical or real-life application? Graphene springs to mind.
Why do I mention this? Well it is the issue of Masks, yet again. I popped into town this morning to do some shopping. A wide range of shops were open, certainly not just grocery stores and pharmacies. Schools have been closed for weeks; public gatherings in cinemas, sports, entertainment and religious events have been suspended, and individual services such as hairdressing, massage and beauty treatments have been closed. This is not a lockdown and not even social distancing. The very concept of social distancing is rather impractical for those living in densely populated high-rise estates in communities where public transport is widely used. Everybody wears masks and nearly everyone has a hand sanitiser of some sort to hand. Interesting use of language, verbs and prepositions; to hand, hand to, on hand, hand on, in hand, hand in. Some taxi drivers have bottles of hand sanitiser in their cars for all passengers to use. Some shops have signs, ‘please clean your hands before touching goods’. Parents will be on hand, to spray hand sanitiser on the hands of the young, and children will be on hand to spray hand sanitiser on the hands of the very elderly. Social awareness, caring for others, wearing masks and becoming obsessional about cleanliness. This is not behaviour supported by the science of statistics and probability, this is the behaviour of people who have been through it before.
Yesterday, in Hong Kong, no new cases of coronavirus. Today four new cases, all returnees, from the US or UK. These were caught / identified before they could get into the community. There are impressive screening facilities at the airport in a conveniently located exhibition complex. It is of concern that a couple in their thirties developed symptoms before their flight from the US but managed to escape. The lack of testing in both the UK and the US is a major concern.
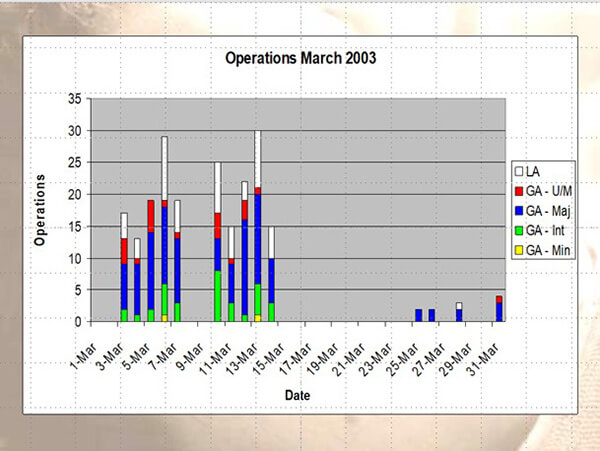
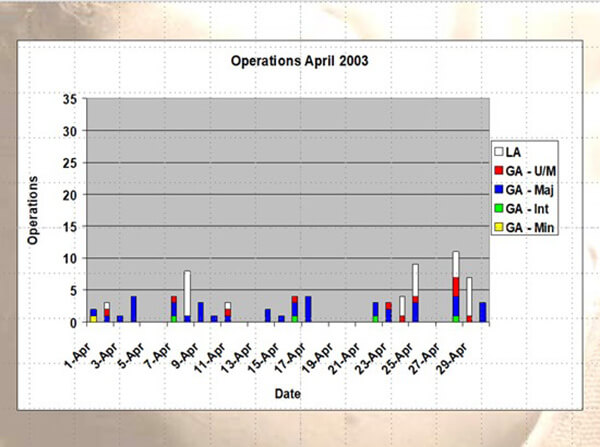
Going back to 2003, life had to go on. From a surgical point of view the problem was not running out of essential PPE, but organising hospitals into ‘clean’ and ‘dirty’. Services are arranged in clinical clusters and in the New Territories East where I was based, we had a major teaching hospital, The Prince of Wales (PWH) in Sha Tin and two other general hospitals with ICU facilities in Tai Po and Fanling. The two graphs show the surgical activity in PWH in March and April 2003. The 15 March being the day that changed things (for ever).
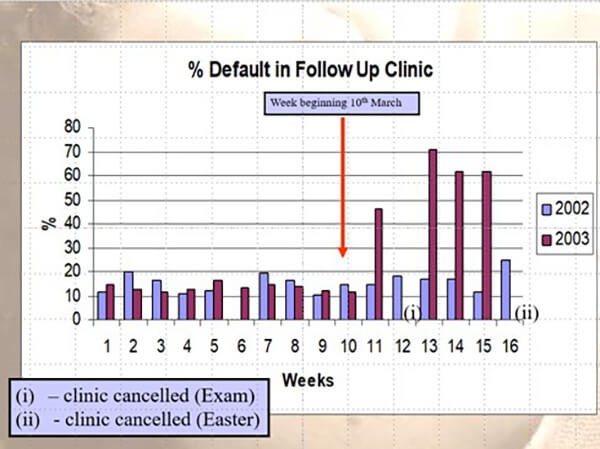
News travels fast in Hong Kong and without mandatory controls, activity and behaviours changed. The following is a slide I used for student teaching which shows the default rate in our plastic surgery follow-up clinics. This was a public hospital clinic, so we were following cases of reconstructive plastic surgery. The general public ‘voted with their feet’. Hospitals were dangerous places, yes, they are, and to be avoided unless absolutely necessary.
Seventeen years on, the responses of both the UK and the USA governments to a global pandemic have been textbook cases of denial, incompetence and blame. Science, per se, is not to blame. In some respects, science is like a computer. It is reactive; the quality of the output depends on the quality of the input and the interpretation of the output depends on the skills and experience of the ‘interpreter’. Three weeks ago, I wrote my first letter from Hong Kong and mentioned two things: fear is okay, and masks are a must. Since then I have been shocked and amazed by the varied responses of world leaders and their advisors. One virus, one human species, why such a diverse global response? Therein lies the paradox of freedom. Democracy demands responsibility and accountability. It is a cruel wake up call to see protesters in the USA demanding the freedom to chose whether they should stay at home or not. “Live free or die” Is a chilling rallying cry.
The WHO has now refined its advice on masks by defining the term medical mask. Click the link and download the advice from WHO: https://www.who.int/publications-detail/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak
“In this document medical masks are defined as surgical or procedure masks that are flat or pleated (some are shaped like cups); they are affixed to the head with straps. They are tested according to a set of standardized test methods (ASTM F2100, EN 14683, or equivalent) that aim to balance high filtration, adequate breathability and optionally, fluid penetration resistance.”
Definitions are good if statements are to be made related to people’s health. We now see the WHO digging in to maintain that the advice they have been giving is “scientifically based”. The CDC has taken the ‘advice’ a step further by using logical reasoning and now favours a cloth-based barrier / mask to limit the transmission of droplets in the general community. There are two lurking threats, the asymptomatic spreader (remember Mary Mallon) and the pre-symptomatic but viral shedding patient. Both threats are significantly reduced if public coughing and sneezing (and even shouting) are limited in their effect to spread (a respiratory) disease.
There are now calls for certain government advisors in the UK to resign: https://www.independent.co.uk/news/health/coronavirus-uk-testing-response-ppe-whitty-jenny-harries-sage-a9474201.html The track record of advice has not been very good. Dithering and massaging the message to fit the political narrative is never a good policy. The UK has failed on the issue of masks and is in danger of failing in the need and practicalities of testing. It is not too late though, if the political leadership is there. A leadership that understands both the importance and the limitations of science and, dare I say it, the role of wisdom in determining action.
Final point, the N95 mask should be the minimum acceptable for frontline health care workers. The use of a transparent face shield is also to be encouraged. I leave you with a picture taken whilst shopping this morning. The transparent shield / mask is now becoming more widely used by the general public in Hong Kong. I took a picture of one in a shop display rather than invade personal privacy! Adapt and survive. Take care out there.

COMMENTS ARE WELCOME


