![]()
As the number of non-surgical options to treat the ageing face has increased in recent years, so have the number of myths about facelift surgery. This article, from two expert facial plastic surgeons from Stanford Hospital in California, provides the truth behind these common preconceptions.
Today, patients have more options than ever before for treatment of the ageing face. These options include laser treatments, injections and traditional surgery. Facelift surgery, traditionally called rhytidectomy, is an extremely popular procedure. In 2016, there were more than 131,000 facelifts performed in the United States, and the number of facelifts is increasing annually. Amongst plastic surgery experts, facelift surgery is the gold standard for rejuvenating the face and restoring a youthful and natural appearance.
As there are so many options besides surgery available to patients, this has led to misconceptions and myths about facelifts. The purpose of this article is to address facelift myths and provide truth to some common misconceptions.
Myth #1: Facial ageing is due to gravity and excess skin
Facial ageing has long been thought to be due to excess skin sagging on the face. Indeed, for decades, the primary method for reversing this has been to tighten the skin by performing skin-only facelifts. Since older facelift techniques focused on repositioning skin only, patients who underwent these (indeed sometimes multiple) lifts obtained an unnatural, stretched appearance. In some cases, the eyebrows and forehead were also pulled upward, giving a startled appearance.
One important aspect of facial ageing that is missed with these is that two other processes are occurring that skin-only facelifts do not address:
- The deeper tissues of the face (fat and muscle) are loosening from their facial attachments and descending, and
- The volume of the face is decreasing. Both bony and fatty atrophy occur with age. Thus, treatments to correct the ageing face should involve repositioning of these deeper structures, and revolumisation, as required.
Modern day techniques focus on both lifting the soft tissue and muscle and restoring volume. Experienced surgeons strive to provide a balanced, natural, youthful look. For example, in a deep-plane facelift, the superficial musculo-aponeurotic system (SMAS) is elevated and resuspended, reversing the effects of gravity. Taking this further, the extended sub-platysmal facelift (technique of the senior author) improves neck contour in a natural way.
Fat transfer is a surgical method for restoring volume to the facial fat compartments. Using this alone or in combination with a facelift can provide optimal results to patients.
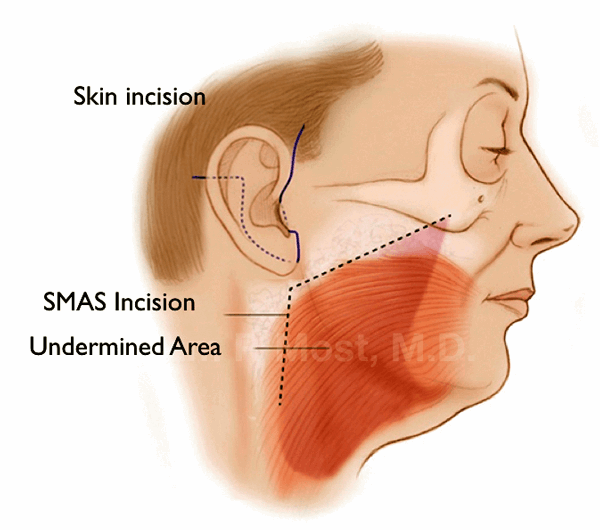
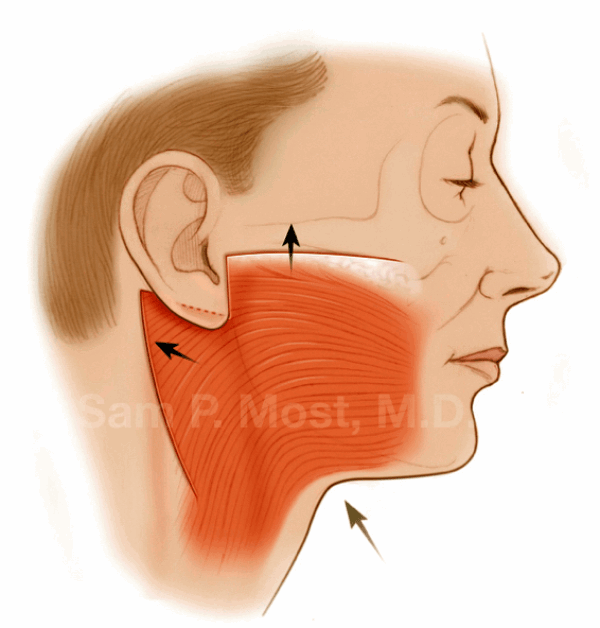
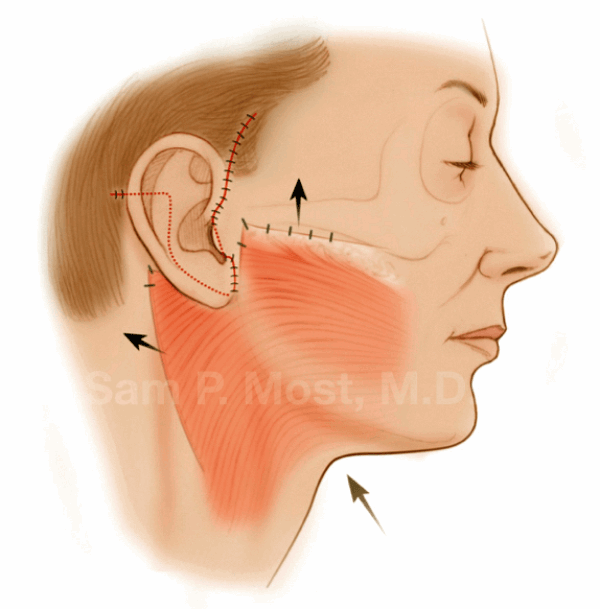
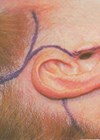
Figure 1: Top image shows skin incision placed in a natural skin crease. The SMAS is incised and undermined. This dissected area is then elevated. The centre and bottom images show the posterior and superior direction of repositioning the face and neck tissues, and these are sutured in place.
Myth #2: Botulinum toxin and fillers (non-surgical facelifts) can achieve the same results as a surgical procedure
While injectable fillers and botulinum toxin have revolutionised the way we treat the ageing face, these do not replace surgical procedures. Rather, they treat signs of ageing that are traditionally treated with a facelift. Facial wrinkles and volume loss are generally not corrected with facelift surgery. This is where the injectables are most useful.
Botulinum toxins act by blocking the neuromuscular junction. This reduces or eliminates the signal from the brain to the muscle, inhibiting movement of the muscle and thus reducing the severity of the associated wrinkles. This neither replaces volume loss which occurs with facial ageing, nor do they treat loose skin, lost muscle or fat displacement.
There is a trend towards filler injections as an alternative to facelift surgery. Facial fillers are made up of various substances (e.g. poly-l-lactic acid, hyaluronic acid, calcium hydroxyapatite) which help restore the lost volume due to atrophy of soft tissue and fat volume that occurs with ageing. Injectables can reduce the appearance of fine lines, shadows, and even add volume to certain areas including the cheeks and lips. However, these results are temporary and for many patients do not provide enough correction of the cheek bones, jawline, jowls and loose neck skin. Fillers still have an important role – they are treatment options for patients who may not be ready for facelift surgery (see Myth #4).
Myth #3: Facelifts are only for women
Men and women equally experience facial ageing and both can benefit from facelift surgery. Demand for male facelift surgery has increased 20% since 2000, while demand for female procedures has remained the same. According to the American Society of Plastic Surgeons (ASPS), in 2016, approximately 12,000 facelift procedures were done on males, which was about 10% of all facelifts done in the USA.
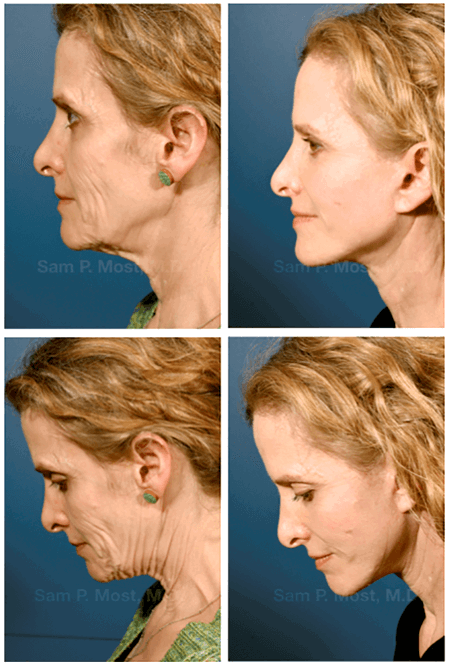
Figure 2: Top row shows before and after profile view for a patient who underwent an extended subplatsymal lift. Note the improvement in jowls, redundant face and neck skin, and facial volume. Bottom row shows before and after neck flexion view with marked improvement in the jawline and neck contour.
Myth #4: You have to be older to have a facelift
There’s no ideal age for a facelift. Although the normal ageing process causes facial skin and underlying muscle to loosen or sag over time, the net effects of ageing can occur at any time. According to the ASPS, the majority of facelift procedures are performed on patients between the ages of 40 to 54 (more than 41,000 in 2015).
Nonetheless, younger people are increasingly presenting to discuss options to maintain their youth. According to the ASPS, patients between the ages of 30 and 39 are particularly interested in forehead lifts and eyelid surgery to remove excess pockets of skin and fat around their eyes. While neither of these procedures are full facelifts, they are still designed to rejuvenate certain areas of the face. It is clear that there is an increasing trend for younger patients to maintain their youth from an early age.
Early onset ageing can be caused by a number of factors: excessive sun exposure, smoking, poor lifestyle habits and genetics are all factors. More importantly, everybody’s skin is different and this impacts the severity of ageing.
We tell our patients that the criteria for being ‘ready’ for a facelift are: 1) Anatomic evidence of facial ageing that is reversible with a facelift, such as jowls, neck skin laxity, or neck bands, 2) Realistic expectations regarding what it can achieve, 3) Good overall medical health and social support. A patient who is 42 may satisfy all three of these criteria, and a patient who is 57 may not.
Myth #5: There’s only one type of facelift
No two patient’s faces are the same. Each patient has completely different facial anatomy and characteristics, facial ageing patterns and goals for surgery. There are many facelift techniques, but the best methods involve repositioning the SMAS, such as the deep-plane facelift or extended subplatysmal facelift. In addition, as mentioned above, volume restoration of the face must be considered for each patient. Many patients also benefit from browlift or eyelid surgery (known as blepharoplasty) in addition to a facelift.
Myth #6: Surgical recovery is long and painful
Historically, facelift recovery was quite painful, and recovery would take several weeks. Today, however, with deep-plane lifting methods, the recovery is shorter (around two to three weeks). Recovery is influenced by how well the patient takes care of their skin after the operation and also the natural healing ability of the individual. Our experience is that many patients feel great after a facelift. The improvement in self-esteem after seeing themselves in the mirror soon eclipses any discomfort.
As with any surgery there is an anticipated process for recovery. Depending on the extent of the facelift procedure and the patient’s medical problems, patients are usually back to their normal activities and work by two weeks. Pain after a facelift procedure is usually limited to the first couple of days after the procedure. Multiple methods of pain control include cooling, elevating the head and postoperative pain medication.
Myth #7: A well performed facelift does not leave scars
All surgical procedures, including facelifts, involve incisions and leave scars. Incisions are typically hidden in natural skin creases and in the hair. When performed by an experienced and meticulous plastic surgeon, facelift incisions usually heal very well and are inconspicuous. In the majority of cases, patients and their friends and family find it difficult to locate the incision weeks after surgery. Scars continue to soften and improve over the course of a year, but never permanently disappear. Additionally, lasers or intense pulsed light (IPL) may take away the redness of the scars earlier instead of waiting months.
Myth #8: A facelift is permanent
After undergoing a facelift, a patient will continue to look years younger than they would had they not undergone the procedure. However, a facelift cannot stop the ageing process and the face will continue to age.
Results vary from patient to patient. Most patients can expect their results to last for seven to 10 years. The longevity of facelift results depends on many variables: history of sun exposure, skin quality, age, smoking history and technique used. Smokers generally have poorer skin quality and elasticity. Older patients will have a quicker onset of postoperative skin laxity compared to younger patients. The deep-plane facelift has been shown to have lower rates of ‘tuck up’, and thus give longer-lasting results.
Genetics also play an important role. If parents aged early, then it is likely the patient will too. General health, diet, drastic weight changes, stressful lifestyle and skin type will all influence the outcome and longevity of the facelift.
Myth #9: Noninvasive facelifts give the same results as a surgical facelift
The holy grail of facial rejuvenation would be a device that allows a patient to get facelift results in the office with no down time. Over the years, various devices have been marketed in this way. Typically these are machines that apply energy to the deep tissues of the face to theoretically ‘tighten’ the loose deep tissue and thus provide facial rejuvenation. The energy types used have been radiofrequency and ultrasound, as well as infrared heating.
Unfortunately, studies have shown none of these devices can achieve results as good as facelifts. The best patients for these treatments are generally those who have minimal signs of ageing and may not be good candidates for facelifting anyway. There is no evidence yet that these devices can ‘stave off’ the need for a facelift later, but this cannot be ruled out yet. The gold standard for treatment of jowls, neck skin laxity and banding remains the deep plane or extended subplatysmal facelift.
“The holy grail of facial rejuvenation would be a device that allows a patient to get facelift results in the office with no down time.”
Conclusion
The goal of modern facelift surgery is to create a natural, rejuvenated look to patients so that they look like a younger version of themselves. The procedure typically involves repositioning of deep fat and muscle tissue and may involve volume replacement. Patients who are not ready for a facelift have several other options, including minimally invasive procedures or injectables.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME