Early facelifting procedures were documented in the 1900s, where skin undermining with excess skin excision along the hairline was performed. The 1970s witnessed a major change with an upsurge in public interest in facelift surgery, which led to innovative changes [1].
The realisation that skin laxity is not the only component in the ageing process, but skeletal changes, deterioration in skin quality and ptosis of the deeper tissues all had a substantial impact fuelled the need for further refinement in facelift surgery [2]. Since then, techniques have evolved with innovations to address the various ageing changes. However, on the backdrop of these numerous described techniques involving a variety of skin incisions, different planes of dissection, and varying approaches of re-draping and skin fixation, it is crucial to adhere to the concept of an optimal facelift [1]. The optimal facelift offers the highest patient satisfaction, sustainable long-term results, with minimal adverse events, along with the lowest morbidity and fastest recovery [3].
Overview
In the early 1970s, Skoog described the subplatysmal plane elevation along the subdermal flap [2]. During the latter half of the decade, the superficial musculoaponeurotic system (SMAS) was defined [2,4]. Then, deep plane and composite facelifts were introduced to address the nasolabial and periorbital areas [2,5]. To further lift the nasolabial area, the malar fat pad suspension was described [6], and subperiosteal rhytidectomy improved results further [7]. However, patients tend to favour less invasive and less complex procedures, therefore the focus has shifted to minimally invasive procedures such as endoscopic lifts, laser skin lifting, with intraoperative adjunctive procedures including the use of radiofrequency, microneedling [8-10] and other heat technology.
Facelift techniques
Subcutaneous and deep subcutaneous facelift
This is one of the first described techniques, effective in minimal ptosis with skin redundancy solely [11]. The dissection is restricted to subcutaneous plane, with supero-lateral draping of skin flap. All the tension is exerted on the skin which results in re-stretching of skin. This issue was overcome with the deep subcutaneous facelift, as the dissection was carried deeper just superficial to the SMAS layer [11-14] (Figure 1).
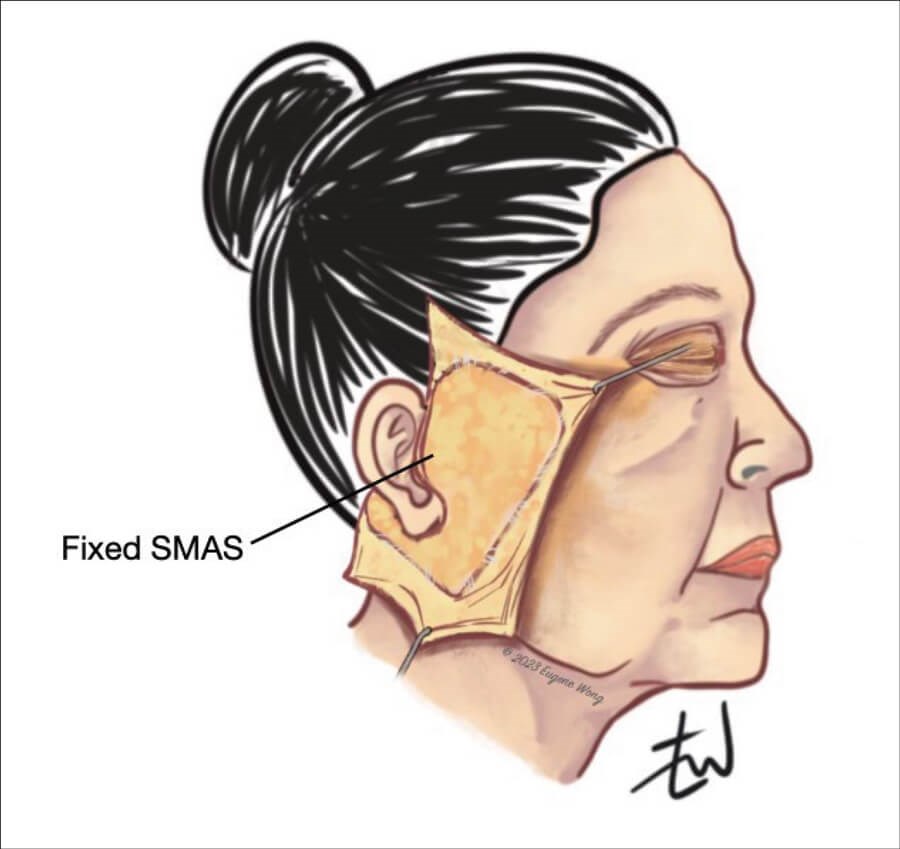
Figure 1: Subcutaneous facelift.
SMAS plication facelift
As the above technique did not address mobile SMAS, the concept of SMAS plication was popularised, to relocate the ptotic fat and mobile SMAS from the lower face to higher level up to the point where the sutures are anchored to the fixed SMAS (SMAS overlying the parotid gland). This suture plication generates infoldings of the superficial fat as it is applied where necessary [15,16]. The drawbacks of this technique are the risk of short-term results because of suture failure and the tethering effect as the retaining ligaments are not addressed in this approach.
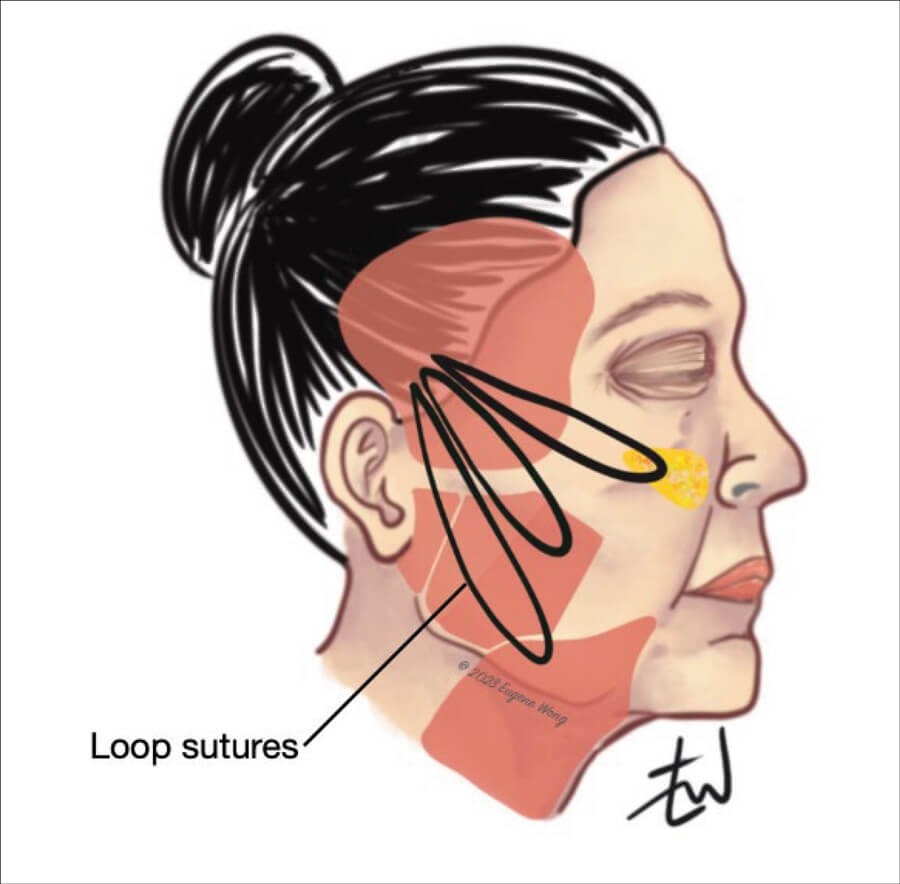
Figure 2: Minimal access cranial suspension (MACS) facelift with loop sutures.
Minimal access cranial suspension (MACS) lift
MACS lift involves suture loops on the SMAS, which are anchored to the deep temporal fascia just superior to the zygomatic arch and anterior to the ear [2,15,17,18] (Figure 2). The skin is re-draped vertically. The skin incision is short, and this is suitable for individuals with little or no skin excess, with minimal jowling and ptosis of facial tissues. Variations in technique may be used to extend its indications.
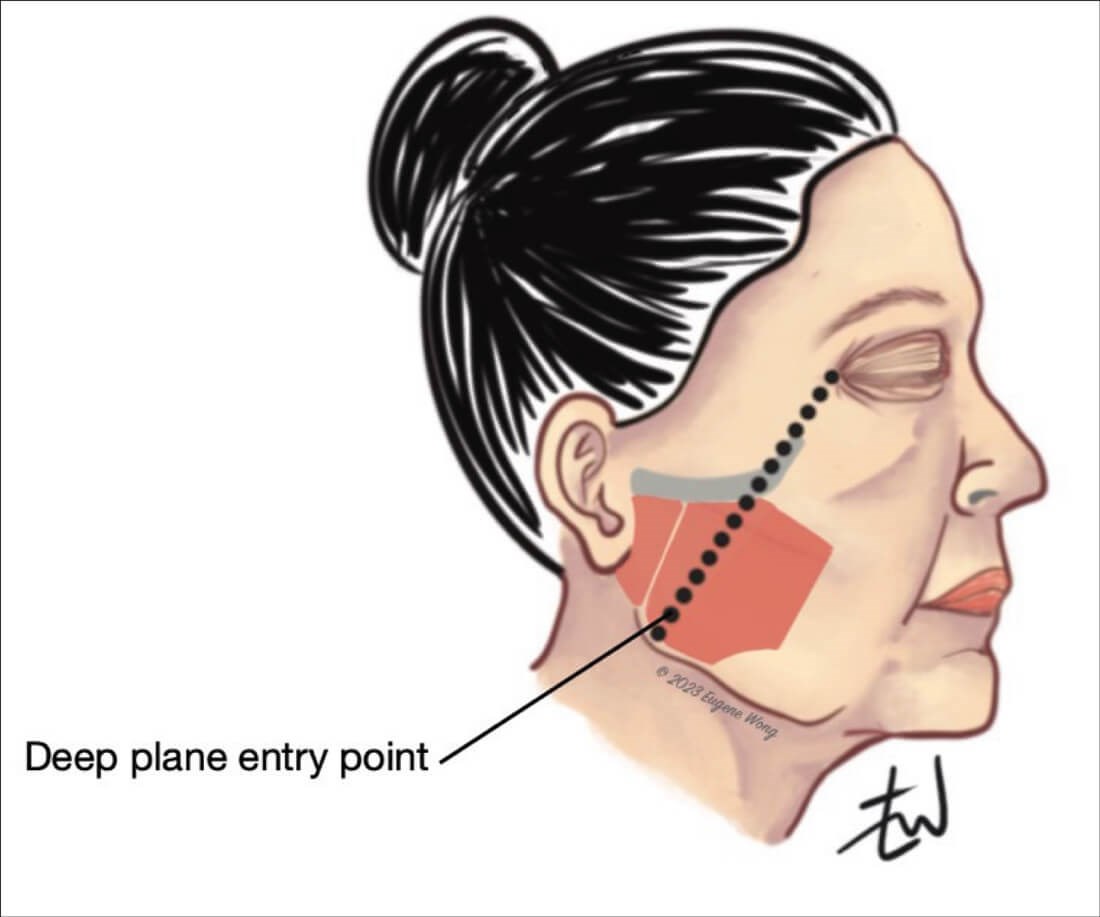
Figure 3: SMAS flap with skin attached (deep plane facelift).
Deep plane facelift (DPFL)
DPFL is suited for individuals with significant ageing of the midface and mento-labial folds and lower face, in which reversal of the ageing changes requires addressing deeper soft tissue. Sub-SMAS is the predominant dissection plane, with the release of facial retaining ligaments (orbital, zygomatic, masseteric, zygomaticus major muscle ligamentous attachments to skin). The elevated flap in this technique consists of skin and subcutaneous tissue, and the malar fat pad is re-draped as necessary [2,19-21] (Figure 3).
Extended SMAS facelift
The difference in this technique is that elevation and re-draping of the skin flap and SMAS are done independently of each other. First, the skin is elevated in the subcutaneous plane exposing the fixed SMAS up to the anterior border of the parotid gland. SMAS is incised along the line drawn from the lateral canthus to the angle of mandible and the dissection is continued in the sub-SMAS plane. The dissection is often extended into the neck in a subplatysmal plane creating a SMAS‐platysmal flap [2,22]. The deep tissues are then elevated and secured using a combination of vertical and posterior vectors, as necessary. The skin is then re-draped without tension.
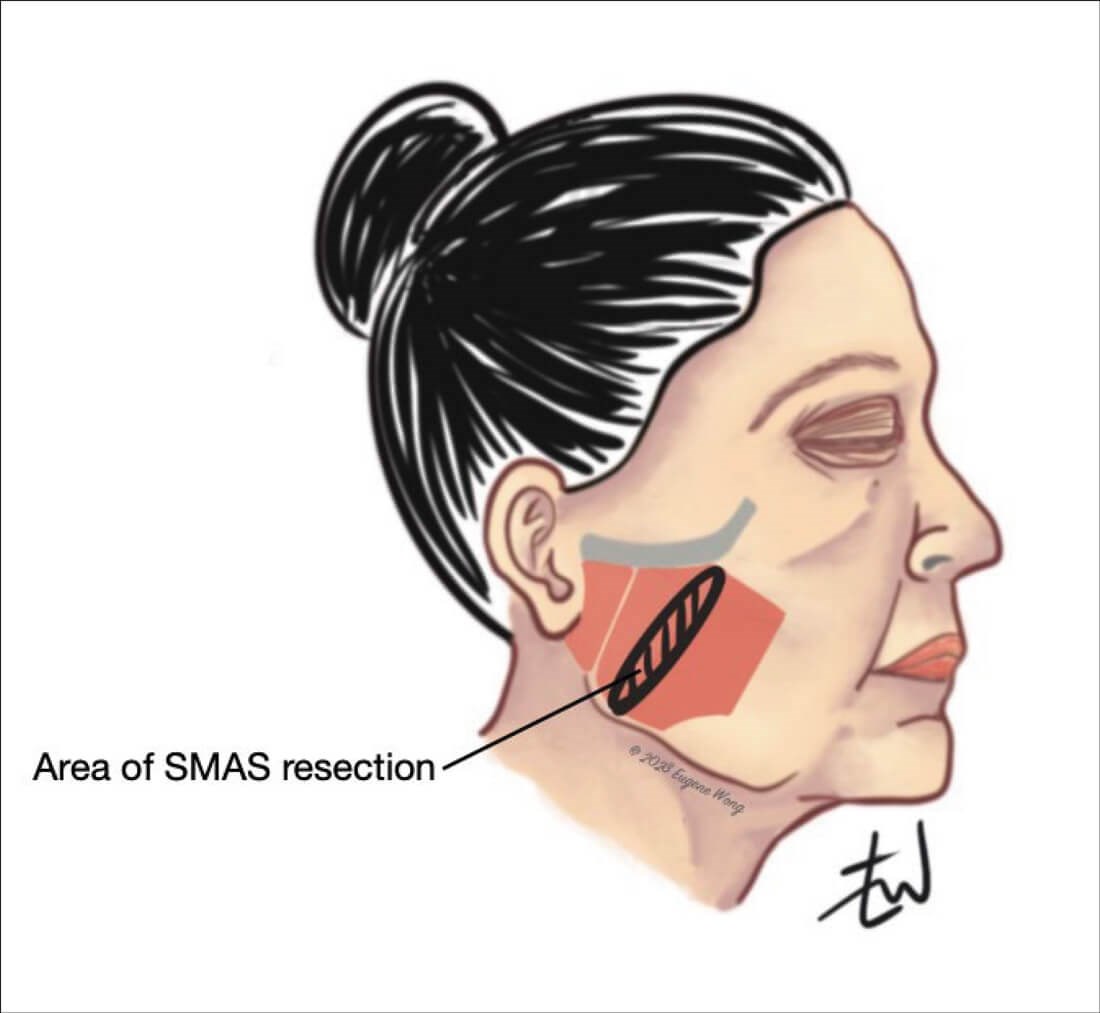
Figure 4: Lateral SMASectomy.
Lateral SMASectomy
This technique involves supra-SMAS dissection, excision of loose and redundant SMAS anterior to the parotid and anchorage to the fixed SMAS posteriorly [19,23,24], reducing redundancy and skin excision as required (Figure 4).
Subperiosteal facelift
This approach is most suitable for patients with significant ageing changes. A temporal incision is used for the sub-periosteal dissection, and the targeted structures are then suspended and sutured to the deep temporalis facia. It can also be undertaken intra-orally and endoscopically. This procedure is recommended for the correction of the ageing changes of the upper and mid-face with excellent results, however it has fallen out of favour because of prolonged oedema and slow recovery [15,25,26].
Non-surgical skin rejuvenation and facelift
Combining surgery and non-surgical measures of a varying degree of invasiveness is becoming increasingly popular [2,27]. However, appropriate patient selection is highly recommended. Radiofrequency (RF) can be used for a non-surgical facelift or as an adjunct following or during surgery. It helps achieve gradual skin tightening by targeting the deep dermis and subcutaneous tissues, by introducing uniform volumetric heating [2,28]. Ablative lasers (CO2 and Er Yag) are also effective particularly for improving skin quality by treating fine lines and other ageing changes [2,29]. Newer devices provide a combination of RF and laser treatments, performed simultaneously, which are effective and easy to use with high patient satisfaction. Other non-surgical techniques which can work in synergy with surgery include micro-needling, injectable fillers, use of fat (milli-fat, micro-fat, nano-fat), platelet rich plasma / fibrin [2,30].
Conclusion
Surgical facelift techniques will continue to evolve along with the increasing role of minimally invasive techniques in improving overall results. Innovative minimally invasive approaches can help in the restoration of a youthful face with natural results and less downtime. It is important that every surgeon involved in facelift surgery should have a variety of techniques in their armamentarium to optimise results for patients.
References
1. Thorne CH. Grabb and Smith’s Plastic Surgery, Sixth Edition. Philadelphia, USA; Lippincott Williams & Wilkins: 2007.
2. Pourdanesh F, Esmaeelinejad M, Mehrshad Jafari S, Nematollahi Z. ‘Facelift: Current Concepts, Techniques, and Principles’. In: Motamedi MHK (Ed.). A Textbook of Advanced Oral and Maxillofacial Surgery Volume 3. InTech Open: 2016
https://doi.org/10.5772/63150 2016
[accessed 27 June 2023].
3. Chang S, Pusic A, Rohrich RJ. A systematic review of comparison of efficacy and complication rates among face-lift techniques. Plastic Reconstr Surg 2011;127(1):423-33.
4. Mitz V, Peyronie M. The superficial musculoaponeurotic system (SMAS) in the parotid and cheek area. Plast Reconstr Surg 1976;58:80-8.
5. Hamra ST. The deep‐plane rhytidectomy. Plastic Reconstr Surg 1990;86:53-61.
6. Owsley JQ Jr, Zweifler M. Midface lift of the malar fat pad: technical advances. Plastic and Reconstr Surg 2002;110:674-85.
7. Ramirez OM. The subperiosteal rhytidectomy: the third generation facelift. Annals of Plastic Surgery 1992;28:218-32.
8. Wei B, Duan R, Xie F, et al. Advances in face-lift surgical techniques: 2016–2021. Aesthetic Plastic Surgery 2023;47(2):622-30.
9. Dayan E, Burns AJ, Rohrich RJ, Theodorou S. The use of radiofrequency in aesthetic surgery. Plast Reconstr Surg Glob Open 2020;8:e2861.
10. Floyd EM, Sukato DC, Perkins SW. Advances in face-lift techniques, 2013-2018: a systematic review. JAMA Facial Plastic Surgery 2019;21(3):252-9.
11. Warren RJ, Aston SJ, Mendelson BC. Face Lift. Plastic and Reconstr Surg 2011;128(6):747e-64e.
12. Joseph J. Hangewangenplastic (Melomioplastik). Deutsch Med Wochenschr 1921;47:287-8.
13. Bames HO. Truth and fallacies of face peeling and face lifting. The Medical Journal and Record 1927;726:86-7.
14. Bettman AG. Plastic and cosmetic surgery of the face. North-west Med 1920;91:205-9.
15. Warren RJ. ‘Facelift: Introduction to deep tissue techniques.’ In: Neligan PC (Ed.). Plastic Surgery: Volume 2: Aesthetic Surgery, 4th Edition Philadelphia, USA; Elsevier: 2017.
16. Robbins LB, Brothers DB, Marshall DM. Anterior SMAS plication for the treatment of prominent nasomandibular folds and restoration of normal cheek contour. Plast Reconstr Surg 1995;96(6):1279-87.
17. Verpaele A, Tonnard P, Gaia S, et al. The third suture in MACS‐lifting: making midface‐lifting simple and safe. Journal of Plastic, Reconstructive & Aesthetic Surgery 2007;60:1287-95.
18. Tonnard P, Verpaele A, Monstrey S, et al. Minimal access cranial suspension lift: a modified S-Lift. Plast Reconstr Surg 2002;109:2074.
19. Hashem AM, Couto RA, Surek C, et al. Facelift part II: surgical techniques and complications. Aesthetic Surgery Journal 2021;41(10):NP1276-94.
20. Jacono A, Bryant LM. Extended deep plane facelift. Clinics in Plastic Surgery 2018;45(4):527-54.
21. Gordon NA, Adam SI 3rd. Deep plane facelifting for midface rejuvenation. Clinics in Plastic Surgery 2015;42:129-42.
22. Ivy EJ, Lorenc ZP, Aston SJ. Is there a difference? A prospective study comparing lateral and standard SMAS face lifts with extended SMAS and composite rhytidectomies. Plastic and Reconstr Surg 1996;98:1135-43.
23. Baker DC. Lateral SMASectomy, plication and short scar facelifts: indications and techniques. Clin Plast Surg 2008;35(4):533-50.
24. Baker DC. Minimal incision rhytidectomy (short scar face lift) with lateral SMASectomy: evolution and application. Aesthet Surg J 2001;21(1):14-26.
25. Tessier P. The subperiosteal facelift. Ann Chir Plast Esthet 1989;34:193.
26. Psillakis JM, Rumley TO, Camargos A. Subperiosteal approach as an improved concept for correction of the aging face. Plast Reconstr Surg 1988;82:383.
27. Centurion P, Romero C, Olivencia C, et al. Short‐scar facelift without temporal flap: a 10‐year experience. Aesthetic Plastic Surgery 2014;38:670-7.
28. Ruiz-Esparza J, Gomez JB. The medical facelift: a noninvasive, nonsurgical approach to tissue tightening in facial skin using nonablative radiofrequency. Dermatologic Surgery 2003;29:325-32.
29. Alexiades‐Armenakas M. Laser skin tightening: non‐surgical alternative to the face‐lift. Journal of Drugs Dermatology 2006;5:295-6.
30. Weinkle A, Sofen B, Emer J. Synergistic approaches to neck rejuvenation and lifting. Journal of Drugs in Dermatology 2015;14:1215-28.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME