
Facial ageing is a complex process which is multifactorial, involving loss of bony support, elongation of the facial ligaments, displacement of fat compartments, attenuation of the superficial muscular aponeurotic system (SMAS) layer and thinning of subcutaneous and dermal tissue. This results in descent and wrinkling of the facial skin.
The process of volumisation without reinforcing the support of the facial tissues will inevitably create an unnatural and distorted facial contour. Volumisation alone does not address the problems of soft tissue descent; the ‘overfilled’ face is commonly seen as a vain attempt to address the soft tissue laxity.
When the underlying anatomy is examined in detail, it is clear that the true retaining ligaments play a crucial role in the architecture of the facial network. These ‘True’ ligaments form fibrous columns which run from the periosteum through the SMAS and branch out to the subcutaneous layer of skin, suspending all the overlying facial layers. Elongation of the true ligaments will result in descent of the overlying tissues and hence sagging of the skin.
The True Lift™ is a non-surgical procedure that focuses on retightening of the true retaining ligaments. This is achieved by placing a high G filler at the base of the ligament, resulting in a direct tightening of ligaments and an indirect lifting of the SMAS layer by a ‘cantilever’ effect.
There are four major facial true retaining ligaments that form the main architectural suspension structures of the face: orbital retaining ligament (ORL), zygomatic retaining ligament (ZRL), buccal-maxillary retaining ligament (BMRL) and mandibular retaining ligament (MRL).
These ligaments are clearly shown in the cadaver dissection for their differences in width and thickness where the placement of the product is required for each ligament in order to obtain the optimum lifting results (Figures 1-4).
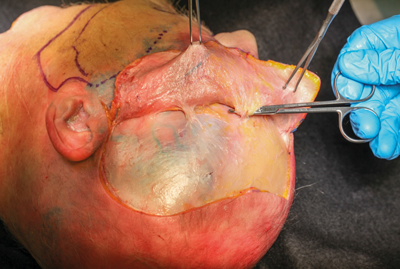
Figure 1. Orbital retaining ligament.
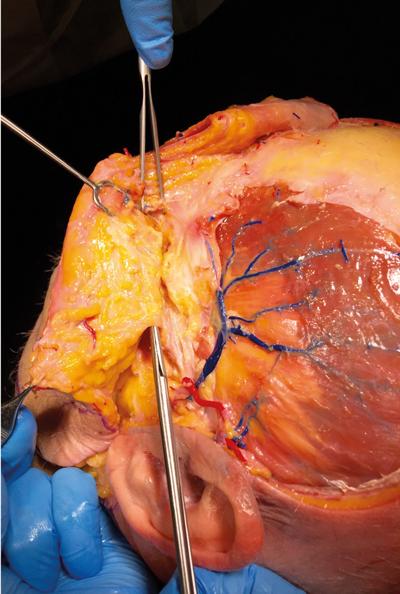
Figure 2. Zygomatic retaining ligament.
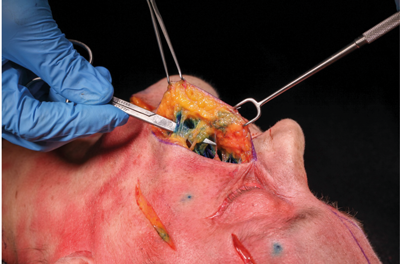
Figure 3. Buccal-maxillary retaining ligament.

Figure 4. Mandibular retaining ligament.
Procedure technique
The points of injection are identified by the palpable indentations on the bone which are the origin of the ligaments (points 1-3, Figure 5). Point 1: The orbital retaining ligament is identified as an indentation on the supraorbital ridge medial to the temporal crest and lateral to the supraorbital foramen and vessels. The indentation represents the point of origin of the ORL.

Figure 5. True lift injection points.
Points 2 and 3 represent the ZRL. Point 2 represents the point of origin between zygomaticus minor and major. Point 3 is lateral to zygomaticus major and medial to the masseteric insertion on the zygoma. This can be clearly seen and palpated if the patient opens their mouth widely.
The injection technique for orbital (point 1) and zygomatic retaining ligaments (points 2 and 3) involves elevating the skin and soft tissues at these points to expose the base of the ligaments. A bolus of 0.1-0.2ml of product is injected perpendicular to the periosteum using a sharp needle to ensure accurate placement at the base (origin) of the ligaments. The overlying skin and soft tissues are released gently, a tenting effect and elevation of the skin and soft tissues should be observed after allowing the tissues to descend gently.
Injection at the base of the buccal-maxillary retaining ligament (point 4), does not require any additional elevation of the skin and soft tissues in this region. A bolus of product is placed at the base of this ligament. This may be approached with a needle at a 45 degree angle to the canine fossa. This injection supports the BMR ligament and volumises the deep medial cheek fat which provides further support and projection of the mid-face.
The mandibular retaining ligament (point 5), is treated similar to the BMR ligament (point 4). The bolus injection is placed at the base of this ligament just medial to the Marionette line near the base of the mandibular border. This injection point elevates the marionette line and further contours the medial cheek and lateral mental border (Figure 5).
The ‘True’ Lift allows the practitioner to address the structural descent of the soft tissues due to facial ligament laxity. Once treated with these small bolus injections it is then possible to continue to treat the bony deficits and volumisation required to rejuvenate the face. The True Lift is based on treating the anatomical changes observed in the facial soft tissue support and forms the basis of treating the deep tissues and building up the facial tissues.

Figure 6. Immediate lifting of right side after true lift.
Immediate tightening of skin and better contour can be achieved with True Lift injection technique using only one syringe (1ml of filler) per side (Figure 6).
This injection technique introduces a simple and effective way to rejuvenate the ageing face. Most importantly, it is a procedure based on the anatomical structure with a predictable result.
COMMENTS ARE WELCOME


