
Detailed knowledge of the anatomy is important prior to any surgical or non-surgical intervention in this complex area. Dr Samizadeh takes us through her pre-procedure analysis.
The most frequent location for faciaaestheticl volumising procedures is reported to be the lips [1-4]. The lips are a key component of the face, and have significant functional roles in: mastication, speech, phonetics, oral seal, a soft tissue boundary for dentition, facial aesthetics, facial expression, tactile sensory organ and are also an erogenous zone [5-7].
Lip augmentation can be carried out surgically or non-surgically, with the latter becoming very popular in recent years. Various types of dermal fillers are commercially available, amongst which hyaluronic acid is currently the most widely used material due to its degradability and good safety profile.
Indications for lip augmentation include the following [8]:
- Medical
- Aesthetic
- Enhancement
- Correction of lip symmetry
- Enhancement of volume and fullness
- Improvement of lip definition
- Rejuvenation
- Ageing
- Genetics


Figure 1: Changes in lip morphology with ageing: Loss of fullness and projection, increased upper lip length, flattening and widening of the Cupid’s bow, loss of philtrum columns, perioral rhytids, loss of vermilion border, lengthening of the cutaneous upper lip. Source: Shutterstock
The perioral region and the lips have a complex anatomy. Hence, knowledge and understanding of the precise structure of the subcutaneous tissue, vascular supply and changes which occur with disease and ageing (Figure 1) are required for carrying out safer non-surgical enhancement of the lips. The following article aims to provide overall guidance on these topics; however, it is beyond the scope of this article to thoroughly discuss all of these factors in depth. For a thorough understanding of evidence-based findings and systematic analysis, the interested reader should refer to Dr Naini’s papers and his reference book Facial Aesthetics: Concepts and Clinical Diagnosis.
Youthful lips are characterised by [5,9]:
- Fullness of upper and lower lips
- Positive vector of the oral commissure
- Well-defined philtrum columns
- Increased visibility of the wet-dry border
- Lip curvature on lateral view
- Central cutaneous lip: anterior projection
- Less acute angle from the commissure to the peak of the Cupid’s bow
Morphological changes with ageing include [5,10,11]:
- Loss of fullness
- Loss of projection
- Increased upper lip length
- Flattening of the Cupid’s bow
- Widening of the Cupid’s bow
- Flattening and loss of philtrum columns
- Reduced vermillion exposure
- Reduction and loss of vermillion border
- Lengthening of cutaneous upper lip
- Increased resting tone of the muscle
- Development of perioral rhytids
- Lower lip may develop ptosis, resulting in lower dental show
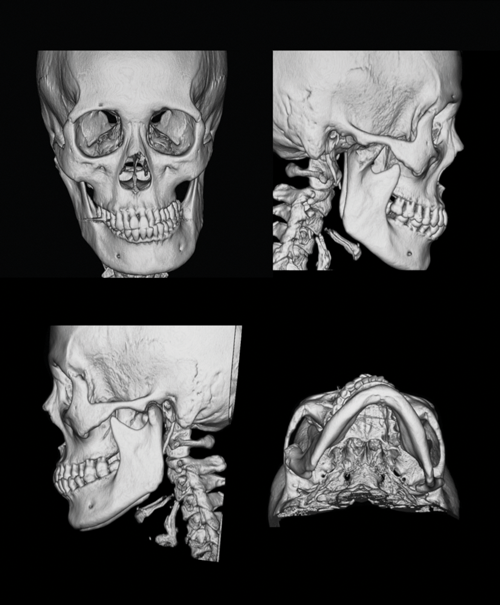
Figure 2: Computed tomography (CT) scan of facial bone 3D, case of facial asymmetry, a 56-year-old female. Maxilla, mandible and the dentition are the skeletal support for the soft tissues of the midface, lower face and the lips. Source: Shutterstock
Assessment
It is essential to assess the parameters, units and relationships between units and subunits that result in ideal proportions and an attractive smile. A thorough understanding and assessment process will result in a better understanding of the aesthetics of the lips and consequently a more successful treatment plan and outcome. Patients should be examined in natural head position at rest and while animating. The maxilla, mandible and the dentition directly and indirectly affect the position of the lips [13] (Figure 2). In addition, it is paramount to keep in mind that the lips are only one factor of an attractive smile.
The components of an attractive smile that should be examined prior to treatment [14] (Figure 3):
- Skeletal components
- The relative position of the mandible to maxilla
- The dentitions, gingivae and alveolar bone - Soft tissue factors
- The lips
- Soft tissue morphology
- Prominence of the chin
- Prominence of the nose

Figure 3: A young man with well supported lips and an elder edentulous gentleman with lack of support for the upper and lower lips. Source: Shutterstock
Skeletal components
The relative position of the maxilla to mandible plays an important role in facial profile aesthetics, and those of the lower face and lips. For example, discrepancies between the maxilla and mandible can result in a concave or convex facial profile. Furthermore, a retrognathic mandible or maxilla can make lip seal difficult [5].
Dentoalveolar components
The inclination of the maxillary and mandibular incisor dentition and dentoalveolar inclination (distance of the dentoalveolus to the respective lip) directly affect the soft tissue profile of the lips. The dentoalveolar protrusion and retrusion is different from maxillary or mandibular retrusion and protrusion. As an example, protrusion of the dentoalveolar can result in disproportionate prominence of the lip. Proclination of the upper teeth can have the same effect on the lip, in particular, if the lip is not thick. In the presence of a true sagittal deficiency of the mandible, the lower lip is everted and hides behind the maxillary incisors, and the mentolabial fold appears accentuated [5].
Dr Farhad Naini has published an ideal and systematic clinical evaluation of the lips [5]. This is recommended to be adopted by all aesthetic practitioners prior to treatment planning and execution.
The acronym LAMPP can be used (Dr Farhad Naini) [5]:
- L: Lip lines
- A: Activity (function)
- M: Morphology (form)
- Lip height
- Lower lip / chin height
- U and L vermillion height
- Lip thickness
- Lip contour and posture - P: Posture
- Normal muscular tone without excessive muscle contraction at rest - P: Prominence
- In relation to the nose and the chin.
Lip lines
The vertical position of the lips relative to the anterior (front) teeth determines the lip lines. In an ideal situation, the upper lip covers the upper anterior teeth, exposing only 2-3mm of the incisal edges and the lower lip covering the lower teeth completely. Lip closure is done with little to minimal contracture. Excessive exposure of the upper anterior teeth and the gums can result in the appearance of a ‘gummy’ smile. A high or low lower lip line can result in retrusion or protrusion of the upper incisor teeth [5]. A high lower lip line can result in more eversion of the lower lip in comparison to the upper lip and a deep labiomental angle.
Lip activity
Examining lip function at rest and during animation is critical, in particular when treatment planning for lip enhancement. Hypertonicity or hypotonicity of the lips can affect the choice of dermal fillers. In hypertonic lips, there is higher chance of nodule formation if the chosen hyaluronic acid dermal filler has high cohesivity and poor tissue integration. In addition, displacement of the product may also be an issue. In cases of underlying deformity (dentoskeletal), it would be preferable to refer the patient for correction that allows normal lip function [5]. The anterior oral seal should also be examined. Exaggerated mentalis muscle contraction for an anterior oral seal would affect the position of the upper and lower teeth and hence the soft tissue morphology of the region [5]. The dentoskeletal relationship affects all above parameters.
Lip morphology
Lip morphology can be examined by analysis of the following parameters while keeping sexual dimorphism and ethnicity in mind [5]:
- Lip height
- Upper and lower lips
- Lower lip / chin height
- Ratio of upper lip to lower lip / chin height
- Interlabial gap (gap between the lips at rest)
- Upper and lower lip vermilion height
Lip thickness
Lip thickness is directly associated with lip prominence and is significantly influenced by ethnic background. Unlike thick lips, thinner lips usually more readily follow the teeth and jaw movements. Lip thickness can be measured from the labial surface (front) of the upper incisors to the vermillion border of the lip [5].
Lip contour
Lip contour should be examined in frontal and profile views to analyse the anterior lip curvature and lip inclination. Lack of dentoskeletal support can result in reduced / diminished or reverse upper lip curvature [5].
“Examining lip function at rest and during animation is critical, in particular when treatment planning for lip enhancement.”
Lip inclination
The upper lip inclination depends on various factors, including the inclination of the upper (maxillary) incisors, the tonicity and thickness of the soft tissue of the upper lip, and also on the space between the dentoalveolus and the mucosal surface of the lip. This inclination varies with age, sex and ethnicity [5,15] and plays an important role in facial profile attractiveness [15,16]. Lower lip inclination is also determined by hard and soft tissue factors including the morphology and posture of the lip, inclination of the lower incisors, and the mandibular dentoalveolus [5].
Lip posture
Lip posture refers to the lip posture and lip seal in natural head position in repose. This will determine the position of the lips at rest and also if the patient has a complete lip seal (can close lips together without excessive contraction of the prioral muscles) or an incomplete lip seal [5,17].
Lip prominence
In profile, the prominence of the lips can be assessed relative to the prominence of the nose and chin. The prominence of the lips can vary due to soft tissue factors such as lip thickness, dentoalveolar factors such as position of the incisor teeth, or skeletal factors [5].
Smile analysis
Smile analysis is an important stage in pre-treatment assessment. An aesthetic smile is dependant on various factors including lip aesthetics (lip lines, lip-maxillary incisor relationship, dynamic upper lip curvature), symmetry and curvature, and the dentition (alignment of the transverse and sagittal occlusal plane, dental midlines, buccal corridors, inclination of the maxillary and mandibular teeth). Assessment should be carried out in both frontal and profile views [5].

Figure 4: Skeletal components including the maxilla, mandible, dentoalveolar, and the dentition provide support for the lips. Superior and inferior labial arteries have a highly variable course and can change layers as they travel through the lips. Source: Shutterstock
Vasculature
The upper lip is mainly supplied by the superior labial artery. Other arterial branches supplying the upper lip include the subseptal arteries and the subalar arteries [18]. The main arterial supply of the lower lip is the inferior labial artery with other arterial branches supplying the lower lip including the horizontal and vertical labiomental arteries [18,19]. It is important to keep in mind that the superior labial artery and the inferior labial artery are absent in some cases. The course of these arteries can be tortuous and highly varied and inconsistent between individuals [20]. Available studies report that the superior labial artery and the inferior labial artery mainly run in the submucosal layer and are not likely to be found subcutaneously (Figure 4). These vessels change layers throughout their course and the superior labial artery is found superficially in the midline [11]. The anatomical heterogeneity in the vascular supply of this region impacts the ability to draw and use landmarks to recommend safe injection depths.
A word of caution
Vascular complications can result from intravascular injection or vascular compression. In rare and severe cases, retrograde injection from the labial arteries to the ophthalmic arteries can result in visual disturbance and blindness. This serious complication is life-changing and practitioners should take all measures possible to prevent its occurrence. The pressure, speed and amount of dermal filler injected play a role in severity of the complications if dermal filler is inadvertently injected intravascularly [21]. Furthermore, although cannulae above 27G reduce the risk of intravascular injection, the risk is not completely eliminated.
Tips to avoid unnatural looking lips:
- Avoid augmenting one site or one lip only.
- Intramuscular injections are prone to dislocation by constant muscle movement, and may cause lumping.
- Do not inject a bolus greater than 0.1ml per injection.
- Avoid needle injections in the deep muscular plane.
- Avoid forceful insertion of cannula (usually done to overcome resistance in the muscular plane).
- Injection to be carried out above the orbicularis oris muscle.
- Filler should not be injected deep into the muscle layer.
- Filler should not be injected close to the mucosal side.
The lips represent an important area in facial aesthetics and a detailed knowledge of the anatomy with a thorough analysis of the structure is important prior to initiating any form of surgical or non-surgical intervention.
References
1. Brandt FS, Cazzaniga A. Hyaluronic acid gel fillers in the management of facial aging. Clin interv Aging 2008;3(1):153.
2. Allemann IB, Baumann L. Hyaluronic acid gel (Juvéderm™) preparations in the treatment of facial wrinkles and folds. Clin interv Aging 2008;3(4):629.
3. Bergeret-Galley C. Choosing injectable implants according to treatment area: the European experience. Facial Plast Surg 2009;25(02):135-42.
4. Sarnoff DS, Saini R, Gotkin RH. Comparison of filling agents for lip augmentation. Aesthet Surg J 2008;28(5):556-63.
5. Naini FB: Facial Aesthetics: Concepts and Clinical Diagnosis. Wiley-Blackwell; 2011.
6. Sawhney CP. Reanimation of lower lip reconstructed by flaps. Brit J Plast Surg 1986;39(1):114-7.
7. Ingervall B. Facial morphology and activity of temporal and lip muscles during swallowing and chewing. The Angle Orthodontist 1976;46(4):372-80.
8. Vent J, Lefarth F, Massing T, Angerstein W. Do you know where your fillers go? An ultrastructural investigation of the lips. Clin Cosmet Investig Dermatol 2014;7:191.
9. Rohrich RJ, Pessa JE. The anatomy and clinical implications of perioral submuscular fat. Plast Reconstr Surg 2009;124(1):266-71.
10. Forsberg CM. Facial morphology and ageing: a longitudinal cephalometric investigation of young adults. Eur J Orthod 1979;1(1):15-23.
11. Coleman SR, Grover R. The anatomy of the aging face: volume loss and changes in 3-dimensional topography. Aesthet Surg J 2006;26(1_Supplement):S4-S9.
12. Lemperle G, Anderson R, Knapp TR. An index for quantitative assessment of lip augmentation. Aesthet Surg J 2010;30(3):301-10.
13. Turley PK. Evolution of esthetic considerations in orthodontics. Am J Orthod Dentofacial Orthop 2015;148(3):374-9.
14. Burrow SJ. The impact of extractions on facial and smile aesthetics. Semin Orthod 2012:18(3);202-9.
15. Naini FB, Cobourne MT, McDonald F, Wertheim D. The aesthetic impact of upper lip inclination in orthodontics and orthognathic surgery. Eur J Orthod 2015;37(1):81-6.
16. Khamashta-Ledezma L, Naini FB. Systematic review of changes in maxillary incisor exposure and upper lip position with Le Fort I type osteotomies with or without cinch sutures and/or VY closures. Int J Oral Maxillofac Surg 2014;43(1):46-61.
17. Naini FB. Lip seals. Br Dent J 2010;209(3):106.
18. Crouzet C, Fournier H, Papon X, et al. Anatomy of the arterial vascularization of the lips. Surg Radiol Anat 1998;20(4):273-8.
19. Al-Hoqail RA, Meguid EM. Anatomic dissection of the arterial supply of the lips: an anatomical and analytical approach. J Craniofac Surg 2008;19(3):785-94.
20. Mağden O, Edizer M, Atabey A, et al. Cadaveric study of the arterial anatomy of the upper lip. Plast Reconstr Surg 2004;114(2):355-9.
21. Tansatit T, Apinuntrum P, Phetudom T. A typical pattern of the labial arteries with implication for lip augmentation with injectable fillers. Aesthet Plast Surg 2014;38(6):1083-9.
Declaration of competing interests: The author has acted as a consultant, trainer, or speaker for Allergan Plc, Merz and Galderma.
COMMENTS ARE WELCOME









