
The question whether a cannula or a needle should be chosen for filler injections does not have a straightforward answer. Injection techniques, as well as filler material, cannulas, needles, injection systems, etc. have to be used in a patient specific manner. I will discuss where I feel the use of cannulas makes sense.
Introduction
One can observe a paradigm shift in filler therapies over the past years. To meet the demands of our patients we need to establish new standards in filler injections. More precise and elegant techniques will increase the quality of the aesthetic outcome as well as reduce side-effects and injection-related complications such as pain, swelling, bruising, irregularities and overcorrection. Blunt-tip cannulas with the injection port on the side of the cannula instead of at the tip were designed to eliminate possible complications associated with traditional sharp tip hypodermic needles. This, along with flexibility of the cannula, gives several advantages over the traditional hypodermic needle for certain indications. The cannula slides through the subcutaneous layer of the dermis rather than cutting through tissues and vessels like the traditional hypodermic needle. With less damage, combined with manoeuvrability, filler injections with a blunt-tip microcannula are quick and practically painless [1-4].
Cannula features
When using cannulas, one should understand important features of these auxillary tools. The insertion and / or penetration force, as well as the gliding capacity depend on their manufacturing process: a silicone coating and a dome-shaped tip design will tremendously ease their insertion; manoeuvrability is easier as silicone coated cannulas reduce ‘drag’ during the injection. The wall design has a great impact on the extrusion force of the filler material: a thinner wall provides a relatively larger bore and will reduce extrusion force and ease injectability. Especially in sensitive areas such as e.g. the periorbital area (one should think of the palpebral line) the following facts are preferable: a hub marking to be able to identify the side hole in the cannula as well as the hole being positioned as near to the tip as possible will increase precision in filler placement which is critical for such delicate areas.
Indication-specific cannula technique
Looking at a specific area: the sagged lateral part of the cheeks, in my opinion, using a blunt tip cannula is preferable. There are specific aspects to consider when treating this area. To obtain a smooth, regular and effective lateral lift in this area of the upper cheek, one has to place the filler on a ‘long’ distance (compared for example with another, opposed indication such as the sunken corners of the mouth where the use of a cannula does not really make sense). For this indication, the use of a blunt tip cannula is elegant, as the filler material can be applied in continous threads, even while crossing different anatomical layers based on one entry point, the Zygomatic Arch Entrypoint (ZAE), only (Figure 1).
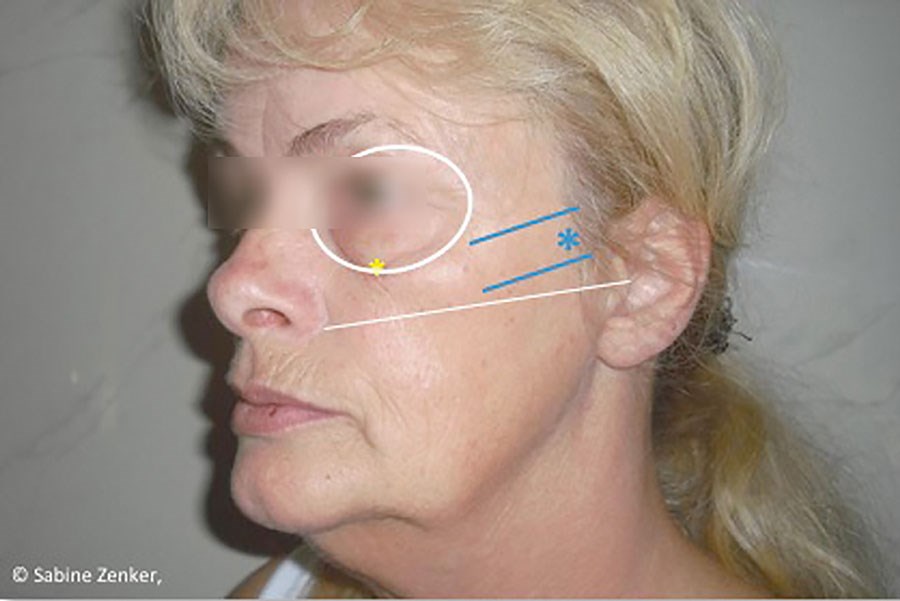
Figure 1 (above left): Zygomatic Arch Entrypoint (ZAE).

Figure 2. (above right).
My technique: sagged lateral part cheeks
The blunt cannula length selected depends on the anatomical parameters (typically from 1½ to 2 inches) with a variety of gauges dependent on the filler (22-27G). The entrypoint is the ZAE. The linear threading technique will be used in a fan-shaped way, covering the whole area of volume depletion by managing the injection from this one entrypoint only.
The filler placement medially will be deep on to the bone (supraperiostally); laterally the filler may end up in the subdermal plane over the zygomatic area.
The volume injected per thread might be approx. 0.1-0.2cc per thread, the goal is to only correct up to the clinical endpoint with gentle molding after injection (Figure 2).


Figure 3: The clinical result, the reshaping and lifting of the lateral part of
the cheeks is illustrated by the black and white photographs.
Conclusion
Using the blunt-tip microcannula is a very elegant and useful technique in specific indications. In my opinion, this produces a very appealing aesthetic result with a precise lifting and provides essential advantages to the patient such as less pain and bruising with far fewer injection points and a notably quicker treatment time.
References
1. Fulton J et al. Filler injections with the blunt-tip microcannula. Drugs Dermatol 2012;11(9):1098-103.
2. DeJoseph LM. Cannulas for facial filler placement. Facial Plast Surg Clin North Am 2012;20(2):215-20.
3. Zeichner JA, Cohen JL. Use of blunt tipped cannulas for soft tissue fillers. J Drugs Dermatol 2012;11(1):70-2.
4. Hexsel D, Soirefmann M, Porto MD, et al. Double-blind, randomized, controlled clinical trial to compare safety and efficacy of a metallic cannula with that of a standard needle for soft tissue augmentation of the nasolabial folds. Dermatol Surg 2012;38(2):207-14.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


