
The Serdev Suture® buttock lift presents a scarless surgical procedure for the treatment of the flaccid, flat and ‘unhappy buttock’ form by a closed approach without any requirement for incision and excision scars. The outcome is a visual change in buttock projection, roundness, tightness and elevates it into a higher position. The buttock lift elongates the lower limbs and changes the proportions of the body.
The aim is to obtain a beautification of the buttock form by creating a circumferential lifting effect on the buttock’s subcutaneous tissue without scars. This is obtained by the use of a suture that takes hold of the inferiorly positioned deep fibrous tissue, elevating and fixing it to the sacro-cutaneous fascia (discovered by the author). This fascia fixes the overlying skin to the lateral lines of the sacrum and suspends the weight of the buttocks. Essential equipment consists of a long, curved, semi-elastic needle and Polycon No 4, 6 or 8 (elastic Bulgarian antimicrobial polycaproamide threads). This operation can be performed either as a standalone procedure or after ultrasonic assisted liposculpture (UAL) that serves to reduce the amount of fat and weight of the buttocks [1-4].
A stable improvement in the buttock position and form was observed in all patients. In the postoperative period the complication rate was minimal and resolved in the first four to five postoperative days. Some pain in the sitting position for at least five to 10 days has been reported. However, all other professional duties, social activities or obligations were possible. This outpatient procedure is effective in the correction of buttock laxity and ptosis. It also creates a new form along with improved body proportions that have been universally accepted as ’happy buttocks’.
Introduction
As more people seek body contouring surgery, we should use our expanding knowledge and surgical experience to create new non-scarring surgical procedures for beautification in areas like the buttocks. Formerly results of body contouring surgery have been less than satisfying. A very small number of techniques are available for correction of the form and the aesthetics of the buttocks. This is especially so for the lax, ptotic and non-projected buttocks. Scarless methods are preferred and demanded by virtually all patients. Classic methods are combinations of liposuction, lipoinjections, implants for augmentation and lipectomy. The outpatient buttock lift procedure by suture can satisfy patients’ requirements for beautification of the buttock form and position without scars. The postoperative period is both short and easily tolerated while the outcome is durable and long-lasting.
Anatomy
The well accepted gluteal position is the location of the gluteus maximus muscle. The muscle-sceletal framework is usually well formed [5]. The female structure often includes an inferiorly positioned fatty tissue deposit, elongating the female buttocks in the inferior perspective [2,4]. Long and hanging buttocks are visible even from a frontal view (Figure 1) and shorten the length of female lower limbs. The hanging buttocks soft tissue is well recognised as ‘unhappy buttocks’ as distinct from the high gluteal position known as ‘happy buttocks’.

Figure 1A: ‘Unhappy’ sagging loose buttock soft tissue, drooping
between the thighs, can lead females to request buttock lifting.

Figure 1B: ‘Happy buttocks’ – the outcome of lifting of the hanging
buttocks is visually elongated legs and more aesthetic body proportions.
Fixation of mobile to immobile tissue
The only useful mobile tissue for suture lift is the very fibrotic buttocks soft tissue. N.B. gluteus muscles and gluteus fascia cannot be lifted. The only immobile structure to which the suture can be fixed in order to produce buttock lifting and secure the buttock weight is the Serdev ‘sacro-cutaneous’ fascia (discovered by the author) which fixes the skin to the lateral edges of the sacrum, located between the ‘dimples of Venus’ at the sacro-iliac points and the upper point of the infra-gluteal fold, located at the sacro-coccigeal point (Figure 2). N.B. Sacro-coccigeal fascia is not useful for fixation. Any attempt to attach the buttocks weight to the sacro-coccigeal fascia can provoke an ‘ischiadic’ pain.
The gluteal fatty tissue is very fibrotic. The fibrotic tissue represents a flexible support for the soft framework of the body [4]. It forms a stable network for subdermal and deep fat layers. We use this stable fibrotic buttock soft tissue structure in order to elevate it securely by fixation to the Serdev fascia on each side.

Figure 2: The Serdev ‘sacro-cutaneous’ fascia fixes the skin to lateral edges of the sacrum in the lower part of the ‘rhombus of Michaelis’. It is located on each side between the ‘dimples of Venus’ and the upper point of the intra-gluteal fold, i.e. between the sacro-iliac points and the sacro-coccigeal point.
Indications
The procedure can be used for: beautification, aesthetic proportions, lifting of ptosis, elongation of the lower limbs, and shortening of the body length in proportion to the legs.
The primary indication for buttock lift surgery by suture is the moderate to severe soft-tissue laxity in the lower trunk with minimal or mild residual fat deposits. In patients with significant fat deposits we initially treat with UAL to reduce the volume and heaviness of the buttock fat tissue. Then we can lift the reduced weight of the buttocks soft tissue and fix it to the Serdev fascia in order to ensure a safe postoperative healing process.
The buttock lift by suture was created for aesthetic purposes with the intention of creating higher and more attractively rounded and projected buttocks, while at the same time creating a visible elongation of the legs and a change of the correlation between body and lower limb length. True buttock sculpting demands a three-dimensional artistic appreciation of the anatomic and surgical adipose layers of the central trunk. This is essential in preventing complications from the buttock lifting where the fixation is done without damaging neurovascular structures.
The technique
The author’s surgical technique consists of a fixation of the complete buttock soft tissue fibrotic system to the sacro-cutaneous fascia each side [4]. The suture technique uses the specially designed Serdev needles from 170 to 250mm, and Polycon No 4, 6 or 8, depending on the degree of tissue volume and heaviness.
The surgeon has to decide which of the perforation points to start from, in what sequence the passes will be done, and in which point to tie the knot. The author prefers the first step for fixation of the subdermal fibrotic tissue to be initiated from the lateral aspect of the buttock. It is easier for beginners to tie the suture at point C (Figure 3). Selection of thread type is the surgeon’s responsibility. However, the elastic tightening of the Polycon suture provides a stable support with a short elasticity when lifting the buttock into a higher position and fixing it to the stable sacro-cutaneous fascia. The suture collects the buttocks fibrotic tissue and its trabecular system into a superficially convex ‘bouquet’. This roundness is moved superiorly and fixed to the sacro-cutaneous fascia. The fixation of the suture to the stable inelastic fascia maximally ensures the longevity of the aesthetic effect. The semi-elastic quality of the antimicrobial polycaproamide suture Polycon (as preferred by the author) reduces the possibility of trauma of the fibrotic tissue and reduces complications.
The buttock lift by suture requires 10 to 15 minutes of operating time per side, no blood transfusions, no stay at the clinic, no nursing care and no more than a day or two off work.
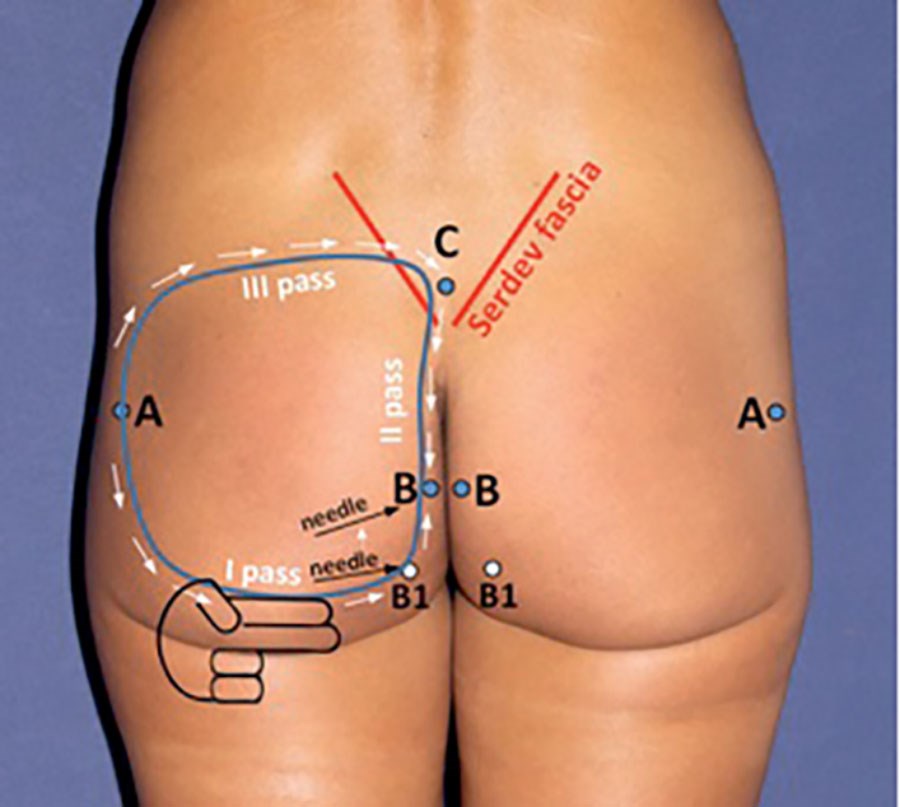
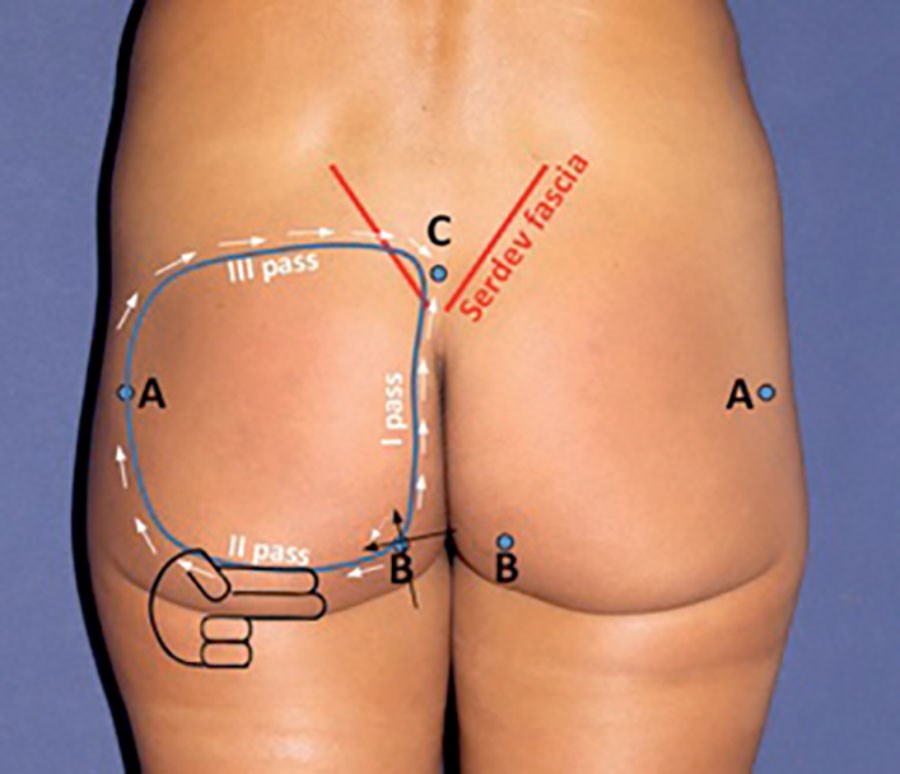
Figure 3: ‘Serdev fascia’ is marked in red colour. It is perpendicular to skin and sacrum and the suture with buttock heaviness will hang on it. Arrows show the direction of needle passes.
A minimum of three passes are necessary to complete fixation of the buttock fibrotic soft tissue system to Serdev fascia, which realises a lift, roundness, projection and stable fixation of the mobile lower buttock to the immobile Serdev fascia. Two methods are presented:
A. First pass from A to B1, then change direction of the needle to B but higher than the anus (B1 is only an orientation, not a skin perforation point). Thread is introduced into B-A. Second pass C-B to take the thread at B. Third pass C-A takes the thread at A and fulfills the circle of the suture at C to be tightened and knotted on Serdev fascia. If no dermis is attached to the suture, all dimples at perforation points are easy to remove.
B. Sometimes it is easier for beginners to perform two passes at once – to start from B to C and introduce the thread from C in direction to B, to change the direction of the needle tip to A without to exit the superficial fascia at B. This manoeuvre prevents beginners from dimpling at point B. After introducing the thread in lines C-B-A, the third pass C-A introduces the thread in line A-C and fulfils the suture circle at C. The suture will be tightened and knotted at C. Dimpling at a perforation point has to be removed.
Directions
Mark skin perforation points A, B1, B and C. Point A should be located lateral at the midpoint of each buttock, near the place where the trochanter can be palpated. This ensures equal distance to points B and C.
Tips and tricks
- Perforation point B could be located above the anus (preferable because of hygienic reasons) or below and somewhat lateral from anus to secure point B from contamination.
- If skin perforation point B is planned higher than the anus, an imaginary point B1 should be taken into consideration and when arriving from point A deep under point B1, the needle direction should be changed to B as shown in Figure 3A.
- If perforation point B is planned below the anus, the superficial fascia at that point B should be perforated very well and widened to avoid perforation with the needle and introduction into the suture. Otherwise its attachment to the suture will produce dimpling.
- Point C should be between both Serdev fascias, inside of the triangle of the sacral region. This will ensure that the passes C-B and C-A both sides will cross the Serdev fascia from below and above and the suture will be fixed to the Serdev fascia. Serdev fascia is perpendicular to skin and sacral edges in the soft tissue and the weight of the suture will be suspended on it.
- Perforation of sacro-coccigeal fascia and fixing the suture on it can produce an ischiadic pain.
- Do not fix gluteus fascia or gluteus muscle to the suture. Both are immobile and will not permit lifting.
After anaesthetic infiltration intradermally and deep in planned perforation points A, B and C, and deep in the soft tissue along the marked suture circle, make small incisions at points A, B and C and open incision and deep subdermal fat in perpendicular fashion with ‘mosquito’ haemostat. Take sterile needle caps from an 18-guage needle, cut part of the closed needle cap tip. Insert these plastic cannulae in twisting perpendicular fashion until maximum depth into perforation points A, B and C in order for the suture to stay deep in the fat fibrotic tissue (near but above the gluteus fascia). Visit http://www.youtube.com/watch?v=mn0O2bNkG7o to access a video of the technique.
First pass A-B
It should be deep in the soft tissue, two fingers higher than the infra-gluteal fold (see Figure 3) in order to stretch and flatten it when the buttock is lifted. Introduce a long Serdev needle 170mm or 230mm from point A to point B1 deep in the soft fibrotic fat tissue. N.B. The Serdev suture circle should be located deep above the gluteus maximus fascia. Be sure not to be too superficial as it will cause skin / tissue dimpling on the way of the needle. If so, twist the needle backwards to free the superficial tissue and proceed deeper. Stay near but above the gluteus fascia, which will block your needle if perforated. Arriving deep at B1, turn the needle to B as shown in Figure 3A. Find the deep positioned opening of the plastic cannula. Go out through the plastic hub. Load needle at point B with a thread No 4, 6 or 8 (depending on buttock size) and pull through. The thread will be located deep in the soft tissue in the mobile line B-A. N.B. Introducing the cannula deeply avoids engaging the dermis and fibrotic tissue in the suture and prevents dimple formation.
Second pass C-B
Proceed from point C to B, deep in the fat tissue, 1-2cm away from the gluteal fold (without superficial skin / tissue dimpling). N.B. If dimpling appears, the needle is too superficially located. Proceed deeper without perforating the sacro-coccigeal fascia (pain!) Find and exit through the plastic hub at point B and load needle. Pull through from B to C. This way the suture has crossed the Serdev fascia medially.
Third pass has two options – A-C or C-A:
Pass A-C: Load needle tip at A. From A, proceed to C – deep subdermally without superficial dimpling and cross lateral through the upper Serdev fascia. Perforate the Serdev fascia near the upper pole and exit at point C through the plastic hub. Unload the needle at C and pull back the empty needle through point A. The suture circle is finalised and both ends of the suture are located at C. Remove cannulae, tighten and knot. Remove dimpling at perforation points. N.B. If you want to tighten the knot at point A, proceed with an empty needle from A to C and load needle at C. Introduce thread at C-A. Then you will have both ends at A. Tightening and knotting the suture at A is somewhat difficult for beginners. Most doctors prefer to knot at C.
Pass C-A: From C, proceed to A, load needle tip at A and unload it at C. Both ends of the suture will be located at C. Remove cannulae, tighten and knot at C. Remove dimpling. Tie the suture as closely as possible to medium tension. This way the whole buttock tissue will be collected and projected like a ‘bouquet’ by the suture and fixed higher to the Serdev fascia. Pull out all dimpling at points A, B and C using a mosquito haemostat.
N.B. Do not perform suture triangles ABC. The higher pressure in the angles will cut the tissue and the suture will become loose. The circle of the suture should be round to apply equal pressure at each point and minimise trauma of the tissue.
The close proximity of the wounds to the anus area makes antibiotic prophylaxis and strict hygiene obligatory.
Warnings
- Do not perforate gluteal fascia or muscle. They cannot be lifted.
- Do not perforate at point C the sacro-coccigeal fascia or periosteum – causes ischiadic pain.
- Make a circular suture to obtain equal pressure around all points. Do not perform triangle sutures – tension on the angles will cut the tissue and produce pain.
Clinical cases
Figure A an B.

Figure C an D.
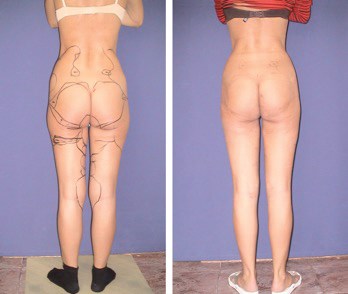
Figure 4A and C: Before UAL and buttock lift; B and D: Day one after ultrasonic liposculpturing of lower extremities, buttocks and flanks and simultaneous buttock lift by Serdev Suture®. Preoperative drawings are still visible. Very rare bruising verifies that surgery has been atraumatic. Tight higher buttocks and straight and elongated legs are demonstrated.
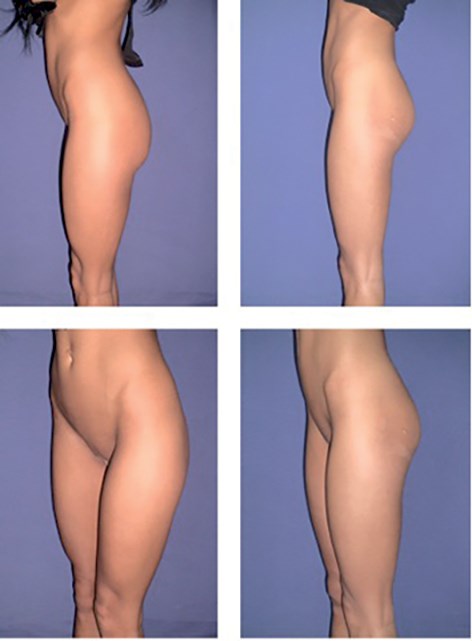
Figure 5: Result after a buttock lift by suture in a dancer. Elongation of the legs is shown. Better projection and higher buttocks are visible even in anterior half-profile position. Profile view: Higher rounded buttock form is achieved. No incision scars persist. The puncture scar 1-2mm in diameter in the lateral area of the buttock isn’t visible.

Figure 6A: Before; B: After buttock lift by Serdev suture. Visible elongation of the lower extremities and shortening of the trunk after buttock lift.
Figure A an B

Figure C an D

Figure 7A and C: Before; B and D: Result after buttock lift by suture in a 62-year-old-patient.
The buttocks are visibly lifted and a better-rounded form is obtained. There is improvement of the whole body shape.
Author’s experience
More than 1000 buttock lifts have been performed by the author in the last 19 years in his clinic and during live surgery workshops around the world in cases of ptotic buttocks between 1993 and 2011. Patients ranged in age from 18 to 62 years. We report our experience with patients followed up to 10 years.
Combined methods
Sixty-three percent of the patients had moderate lower trunk and lower limb cellulite and fat deposits which required additional ultrasonic liposculpture of the lower body and limbs. In patients who have had buttock lift in combination with ultrasonic assisted liposculpture, UAL was performed to reduce the volume and to sculpture the buttocks and other areas for total leg or body beautification. UAL additional positive qualities are skin tightening and weight loss. When using the UAL for buttock sculpturing, our goal is to minimise the fat deposits, buttock’s weight and to obtain a nice rounded and higher positioned buttocks over the gluteus maximus muscle.
Results
As previously stated the buttock lift by suture requires 10 to 15 minutes of operating time per side, no blood loss or transfusions, no stay at the clinic, no nursing care and not more than a day or two off work.
The cosmetic results were evaluated with preoperative and postoperative photographs and by patient satisfaction. No patient was dissatisfied with the results and all of them considered their results as excellent or very good.
Risks and complications
Risks are: higher pressure on one tissue being different from the tension in other areas and points; contamination – skin perforation point B near the anus area. Higher pressure should be prevented by performing a circle – a round form suture that equalises pressure on all points and prevents tension and trauma of the tissue. Infection can be prevented with better selection of point B and antibiotic prophylaxis. The Bulgarian thread is antimicrobial.
In our patients we observed one case with a painful hardness in point B near the infra-gluteal fold and four other cases with a local infection in one of the wounds. The cause for the first complication was the rigid nylon suture that we used in our first patient. The hardness and inelasticity caused tissue trauma in the point of tension on the soft tissue. After this complication we avoided this risk by changing the suture material and we now use the semi-elastic Bulgarian antimicrobial Polycon suture. In all other cases the local infection was easily treated in a matter of days. Infections are very rare occurring mainly at the skin perforation points and are easily treated. No haematoma or nerve damage has been observed. Pain is limited to the first one to two weeks in a sitting position. In limited cases patients forget about or ignore the advice given to commence physical activities gradually. In these few and limited cases abnormal friction and trauma can cause pain that is usually on one side. Palpation along the suture gives information about the location of the pain, usually near a perforation point.
In very rare cases, we have opened the skin perforation scar and some seroma or blood drops have been evacuated with the disappearance of the pain. If there is no infiltration around the suture, slowing down activities, non-steroid anti-inflammatory drugs and painkillers are enough. Antibiotics can be added if considered necessary.
Discussion
There is an increasing demand for surgical correction of the body contour in modern society. There are a limited number of operations that aim to correct non-aesthetic buttock form as part of total body contouring and proportions. The hips, thighs and the lower back frame the buttock contours. Ethnic differences in the shape and proportions of the buttocks create a variety of aesthetic perceptions in size and shape. However, high positioned ‘happy’ buttocks and elongated legs have always been in fashion.
Flat and sagging buttocks are a common clinical condition. However, before the suture butt lift there were no proven aesthetic and effective therapeutic options at hand. Sole excision of skin cannot perform a true lift of the heavy buttocks. Subcision is a surgical technique that is used in treating advanced degrees of cellulite [6]. To treat excesses of fat and skin tissue in that area, liposuction and / or dermolipectomy are mostly used [7]. The indication for liposuction is restricted to the conditions in which the overlying skin is capable to retract and adapt itself to the new contour. If excess skin is the cause of the deformity, a dermolipectomy is mostly indicated [8-15]. Liposuction of the buttock area is infrequently mentioned in the literature and for some authors it is a forbidden zone. Two additional approaches in suction lipectomy of the buttock region are described: liposuction of the ‘banana’ and liposuction of the ‘sensuous triangle’. A common complication of liposuction of this area is ptosis of the buttocks [16,17]. To improve buttock roundness, fat transplantation and different implants, including mammary ones, were introduced [16,18-22]. In trying to achieve symmetry and better contour of the back torso and middle third of the body, the combination of liposuction and lipoinjection has rapidly become known and is a procedure of choice for many authors [16]. Complications are minimal. The quantity of fat infiltrated by most authors varies from 120 to 280cc per gluteus, with a mean of 210cc.
In obese patients the functional benefits of a combination ‘excision-suction’ lipectomy outweigh the disadvantages of the scarring. If there is considerable excess of skin and tissue, excision procedures are performed to remove excess tissue by surgical resection via appropriately large incisions. Resulting scars are visible. Lipectomy with suction of the lower extremities has been practised in recent years. Due to some authors the number of overweight and bariatric patients seeking dermolipectomy of the trunk and thighs is increasing. The so-called ‘lower body lift’ combines the transverse flank / thigh / buttock lift and the fascial anchoring medial thigh lift in one operation. Secondary buttock corrections pose difficult problems because of the poor vascularisation of certain areas, the limited mobilisation of the soft tissue, and the tendency toward poor scar formation. These factors limit the surgical techniques available. The tendency for the deformity to recur may necessitate several corrective procedures. The deep planed torso-abdominoplasty is beneficial for treating gestation sequelae of the torso-abdominal wall, ptosis of the abdomen, vertical and horizontal enlargements of the musculoaponeurotic system, lipodystrophy, stretch marks, rhytidosis of the inguinal region, and ptosis of the external quadrant of the gluteus and the external trochanter area in one surgical procedure. It creates pexy of the external quadrant of the gluteus region [23,24].
Muscle strength is the limiting factor in repetitive lifting. Lower body lift with superficial fascial system suspension is introduced to treat laxity of the entire lower trunk and thigh regions in one stage in selected patients. This procedure needs three weeks off work and is expected to result in a tightening of the flank, buttocks and total thighs. Minor complications are significantly higher than with the component procedures alone and occur in nearly 50% of patients. Another surgical procedure, a circumferential torso excision was designed and utilised for a minimal number of patients [11,12]. This technique dramatically reduces the lateral flank and posterior tissue rolls to improve the operative results. Contour improvement of the buttocks and lateral thighs should be present as well. Belt lipectomy [13] includes the traditional abdominoplasty or panniculectomy with excision extended laterally around the entire trunk. This technique yields a lateral thigh and buttock lift, and when combined with liposuction is used to improve contour of the thighs.
Correction of sequelae of primary hip-buttock-thigh plasty has become a common challenge in aesthetic plastic surgery. Some authors have suggested alternative techniques for dealing with this problem, including denuding the skin at the depressed area, pulling flaps upward and outward, using dermal buried flaps, and utilising liposuction [10,14,16]. Liposuction can be used successfully in combination with classic hip-buttock-thigh plasty to enhance the aesthetic result [16]. Excision body lifts are surgical procedures that are infrequently performed because the length of operating time increases the risk to the patient as well as the likelihood of surgeon fatigue. The other drawback of body lifts is the long incision line. However, these incisions are well accepted if they are well placed and if the results of body change are significant. Meticulous haemostasis, limited undermining, and the closure of dead space are factors that produce a more reliable procedure, both in terms of postoperative problems and the final results [15,23].
In obesity suture lifts are not indicated. The excision surgical procedures are associated with risks. The undesired sequelae of suction lipectomy are contour irregularities, hypaesthesia, oedema, ecchymosis and pigmentary deposits. The potential complications are blood loss, haematoma, seroma, infection, greater saphenous vein thrombosis, fat emboli and skin slough. In excision procedures additional complications are spreading scars as a result of tension, and occasional delayed healing of tense wounds. Excision buttock lifts have not gained widespread acceptance because of problems such as large trauma and blood loss, prolonged postoperative period, early inferior scar migration, and recurrence of ptosis. The most frequent complaint is unacceptable scarring and hypaesthesia. Lipoinjection complications are gluteal temporal hyperaemia and erythema, corresponding to fat necrosis. Acceptance of bodily proportions in races different from those of Caucasians has to be foreseen. Furthermore, Afro-Americans and Asians tend to hypertrophic scarring.
Conclusion
Redundant tissue in sagging buttocks can be corrected by excision lifts. However, these are seldom used procedures because of postoperative problems such as unacceptable inferior displacement, wide scars, early recurrence of ptosis, large trauma, blood loss and a prolonged postoperative period.
In order to limit these complications in flat and sagging buttocks without remarkable fat deposits, we developed a surgical technique using a circumferential suture of the soft tissue to the gluteus fascia. The circumferential suspension gives strong vertical support with minimal tension in each point and reduces the complications traditionally associated with such procedures.
The author’s suture lift operation offers fewer complications than any others described. It is an efficient and safe procedure to correct or enhance buttock contour. It has virtually eliminated blood transfusions and the major complications of liposuction and dermolipectomies under general anaesthesia.
In patients whose problem was excessive fat in conjunction with flabbiness, UAL of the buttocks combined with the buttock suture lift method completed the main goals of the procedure in one or more stages. The combination of UAL and buttock lift by our suture technique is a minimally invasive procedure that can be used to reduce and lift the buttocks at the same time.
The Serdev Suture® buttock lift technique is simple and low in cost with minimal morbidity and very good results. It is important to note that a good result does not depend on great surgery but rather on more simple and acceptable procedures for the patients. Outcomes include harmonious structuring and positioning of the form, lifting of the lower portion of the buttocks, augmentation in the upper gluteus part and better projection. Complications with suture lift of the buttocks are few and patient satisfaction is high. The result is a visual change in the buttock projection, roundness tightness and higher positioning. The buttock lift elongates the lower limbs and visibly changes the proportions of the body. Indicated are patients of regular weight seeking higher, rounded and projected buttocks with better proportions. Heavy buttocks and obesity are contraindicated.
References
1. Serdev NP. ‘Buttock lift. Two own methods.’ Presented at the 3rd International Congress of the South-American Academy of Cosmetic Surgery; Buenos Aires, Argentina; 19-21 October 2001.
2. Serdev NP. Buttocks lift by ultrasonic assisted liposuction: My technique. International Journal of Aesthetic Cosmetic Beauty Surgery 1991;1(3):130-54.
3. Serdev NP. ‘Buttocks lifting without implants - Serdev technique no visible scars.’ Aesthetic Surgery Course; Sofia, Bulgaria; 26 November 2001.
4. Serdev NP. Suture Suspensions For Lifting Or Volume Augmentation In Face And Body (English version). Int J Aesth Cosm 2001;1(1):2561-8.
5. Anikina TI. Soft framework of the human body. Arkh Anat Gistol Embriol 1980;78(3):5-15.
6. Hexsel DM, Mazzuco R. Subcision: a treatment for cellulite. Int J Dermatol 2000;39(7):539-44.
7. Teimourian B, Adham MN. Anterior periosteal dermal suspension with suction curettage for lateral thigh lipectomy. Aesthetic Plast Surg 1982;6(4):207-9.
8. Pitanguy I. Surgical reduction of the abdomen, thigh, and buttocks. Surg Clin North Am 1971;51(2):479-89.
9. Delerm A, Cirotteau Y. Cruro-femoro-gluteal or circumgluteal plasty. Ann Chir Plast 1973;18(1):31-6.
10. Shaer WD. Gluteal and thigh reduction: reclassification, critical review, and improved technique for primary correction. Aesthetic Plast Surg 1984;8(3):165-72.
11. Gonzalez M, Guerrerosantos J. Deep planed torso-abdominoplasty combined with buttocks pexy. Aesthetic Plast Surg 1997;21(4):245-53.
12. Carwell GR, Horton CE Sr. Circumferential torsoplasty. Ann Plast Surg 1997;38(3):213-6.
13. Heddens CJ. Belt lipectomy: procedure and outcomes. Plast Surg Nurs 2001;21(4):185-9, 199.
14. Pascal JF, Le Louarn C. Remodeling bodylift with high lateral tension. Aesthetic Plast Surg 2002;26(3):223-30.
15. Karnes J, Salisbury M, Schaeferle M, et al. Hip lift. Aesthetic Plast Surg 2002;26(2):126-9.
16. Cardenas-Camarena L, Lacouture AM, Tobar-Losada A. Combined gluteoplasty: liposuction and lipoinjection. Plast Reconstr Surg 1999;104(5):1524-31.
17. Lawrence N, Coleman WP 3rd. The biologic basis of ultrasonic liposuction. Dermatol Surg 1997;23(12):1197-200.
18. Chajchir A. Fat injection: long-term follow-up. Aesthetic Plast Surg 1996;20(4):291-6.
19. Agris J. Use of dermal-fat suspension flaps for thigh and buttock lifts. Plast Reconstr Surg 1977;59(6):817-22.
20. Niechajev I, Sevcuk O. Long-term results of fat transplantation: clinical and histologic studies. Plast Reconstr Surg 1994;94(3):496-506.
21. Pereira LH, Radwanski HN. Fat grafting of the buttocks and lower limbs. Aesthetic Plast Surg 1996;20(5):409-16.
22. Peren PA, Gomez JB, Guerrerosantos J, Salazar CA. Gluteus augmentation with fat grafting. Aesthetic Plast Surg 2000;24(6):412-7.
23. Lewis JR Jr. Body contouring. South Med J 1980;73(8):1006-11.
24. Lockwood T. Lower body lift with superficial fascial system suspension. Plast Reconstr Surg 1993;92(6):1112-22.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


