
Botulinum toxin A (BoNTA) is commonly used as an off-label cosmetic modality to improve the ageing lower face and neck, and may be used as a single line treatment or in combination with other procedures, such as dermal fillers [1]. This paper examines the anatomy of the lower face to enhance the clinician’s anatomical awareness, and reinforce the importance of reducing the risk of complications through judicious and accurate placement of product. An analysis of the patient at rest and during animation, with the use of facial aesthetic scales is important to allow the clinician to determine if BoNTA is an appropriate modality for the lower face [2].
There are morphological changes in ageing males and females, as the facial skeleton undergoes significant bone resorbtion [3]. The ramus height and width decreases, while the mandibular angle increases from approximately 90° to 120° [4]. The width and height of the mandible decreases with a reduction of the protrusion of the chin. This is significant when treating a ‘cobblestone’ chin as the mentolabial crease becomes pronounced as the attachment for the mentalis muscle reduces, causing a chronic ‘dimpling’ [5]. Equally, with age, maxillary retrusion contributes to the loss of soft tissue support and medial, inferior migration of subcutaneous fat compartments [6]. The jowl fat increases in volume inferiorly, resulting in formation of the marionette line. The labiomandibular fat pad develops volume loss along the lateral edge, medial to the marionette fold [6]. An awareness of these changes is crucial for the clinician to assess if BoNTA would be a suitable treatment, for the presenting concern.
Masseteric hypertrophy
Kim et al. describe the most prevalent complication in treating masseteric hypertrophy, such as undesired concavities at the lateral aspect of the face and an unnatural smile [7]. In addition, Cavallini et al. describe lip asymmetry, an inability to smile and worsening in the appearance of jowls as key findings from their review [8]. It is suggested that these adverse events occur through inaccurate dosing and placement as a key factor as well as inappropriate patient selection.
The masseter elevates the mandible and has deep and superficial components [9]; the former attaches to the medial border of the zygomatic arch and inserts onto the superolateral mandibular ramus [10]. The superficial head attaches to the inferior and anterior border of the zygomatic arch and also inserts onto the inferior and lateral parts of the mandibular ramus. The muscle is innervated by the masseteric nerve from the mandibular division of the trigeminal nerve. The parotid gland and duct, transverse facial artery and branches of the facial nerve pass superficially to masseter [10]. BoNTA can significantly improve the appearance of a prominent mandibular angle, associated with masseter hypertrophy [1]. A variety of injection techniques are described within the literature. A suggested approach is to place product supraperiosteally, along the inferior aspect of the mandible [9], to reduce the risk of inadvertent placement within the parotid gland, risorius or depressor anguli oris [11]. The parotid gland may vary in size and as such, depth of injection in this region is crucial [9]. Identifying the facial artery is a useful topographic landmark when treating the lower face; arising from the external carotid, it crosses the inferior border of the mandible, where it may be palpated, at the anterior border of masseter [5], the artery is deep to the superficial musculo-aponeurotic system (SMAS), at this location. The point at which the artery crosses the mandible also indicates the posterior border of the depressor anguli oris muscle [11]. Precise dosing to masseter is crucial to prevent asymmetry and unsightly ‘dimpling’ of the muscle.
Depressor anguli oris
Depressor anguli oris attaches from the inferior aspect of the mandible and inserts into the angle of the mouth, some fibres blend and provide origin for orbicularis oris. It depresses the corners of the mouth and is innervated by the buccal and mandibular branches of the facial nerve; it antagonises levator anguli oris [11]. Successful treatment with BoNTA can improve the jawline and pre-jowl area as platysma is contiguous with depressor anguli oris, and as such both muscles may be targeted with a single injection of toxin, supraperiosteally at the inferior aspect of the mandible [11]. This suggested technique is inferior to the modiolus, and as such, should not compromise the chiasma comprising the risorius, orbicularis oris, or zygomaticus major [10]. The modiolus topographically signifies a transition point for the facial artery traversing from deep to the SMAS layer, to reside in the subcutaneous plane, adjacent to the modiolus [5]. The depressor anguli oris is reported to overlap the depressor labii inferioris by approximately 8-10° [11], which emphasises the importance of accurate placement to avoid compromising the lower lip.
Orbicularis oris
Orbicularis oris originates from both the anterior midline of the maxilla and mandible as well as the angle of the mouth where fibres blend with levator anguli oris, depressor anguli oris, zygomaticus major and risorius [12]. The orbicularis oris muscle inserts into the skin along the mouth and is innervated by the buccal and mandibular branches of the facial nerve and allows for closure of the mouth as well as protrusion and pursing of the lips [5]. In suitable individuals portraying dynamic vertical ryhtides, originating from the vermillion border of the lip, low doses of BoNTA may successfully soften the appearance of these. A varying degree of functional impairment when speaking, eating and drinking may occur, which reinforces the importance of an intradermal technique comprising exact dosing of small quantities of toxin, at each injection point.
Mentalis muscle
The paired mentalis muscle originates from th e incisive fossa of mandible and inserts and protrudes the skin of the lower lip and is innervated by the mandibular branch of the facial nerve [11]. A combination of BoNTA and dermal fillers can be effective to correct the age-related ‘cobblestone’ effect and loss of boney support at the anterior aspect of the mandible. These two modalities can provide structural support and smooth the overlying skin, through relaxation of the contracted mentalis. In younger individuals without the loss of support, who display an active mentalis muscle, BoNTA administered as a single treatment may yield a good cosmetic outcome, without the need for additional treatment. A single mid-line injection, deep to the belly of the muscle is suggested to avoid inadvertent placement to depressor labii inferioris, or depressor anguli oris [13].
Platysma
The platysma is a broad flat sheet of muscle, superficial to the deep cervical fascia [10]. It extends from the fascia over the upper parts of pectoralis major and deltoid to the lower border of the mandible, with fibres coursing superiorly to blend with the lower facial muscles. The platysma is innervated by the cervical branch of the facial nerve [14]. With ageing, the platysma begins to lose tone and is pulled laterally, resulting in splaying of the medial fibres. In addition, there is attenuation of the deep retaining ligaments on the medial edge of the muscle contributing to loss of tone. This loss of tone allows the medial edges to descend, leading to development of platysmal bands, which can be exaggerated with contraction [14]. The aim of contouring the neck and jawline with BoNTA is to define the cervicomental angle, as well as smoothing the appearance of the platysma, when contracted [15], and as such, the close relationship of the supra and infrahyal muscles, as well as outer larynx muscles should be respected. Precise, intradermal injection of toxin, along each prominent band is advisable, with varied patterns of placement described within the literature [14,15]. Excessive or inaccurate dosing in this region could have devastating repercussions, such as dysphagia or airway compromise.
Treating the lower face with BoNTA requires not only a sound anatomical knowledge, but also an accurate delivery system to the target muscle. Many conventional syringes do not afford the clinician the necessary level of accuracy required to administer low, precise doses, which is imperative to treat the musculature of the lower face safely and effectively. Errors of dosing may occur to parallax reading, and difficulty in controlling small dose delivery. The 3Dose botulinum toxin syringe is one way to avoid these errors. It is designed to be compatible with the three current Food and Drug Administration (FDA) approved toxins and allows the clinician to reconstitute and administer accordingly. Each delivered dose is exact and administered as an audible tactile ‘click’ to allow the clinician to focus on the patient and area being treated. The syringe also expels all residual toxin.
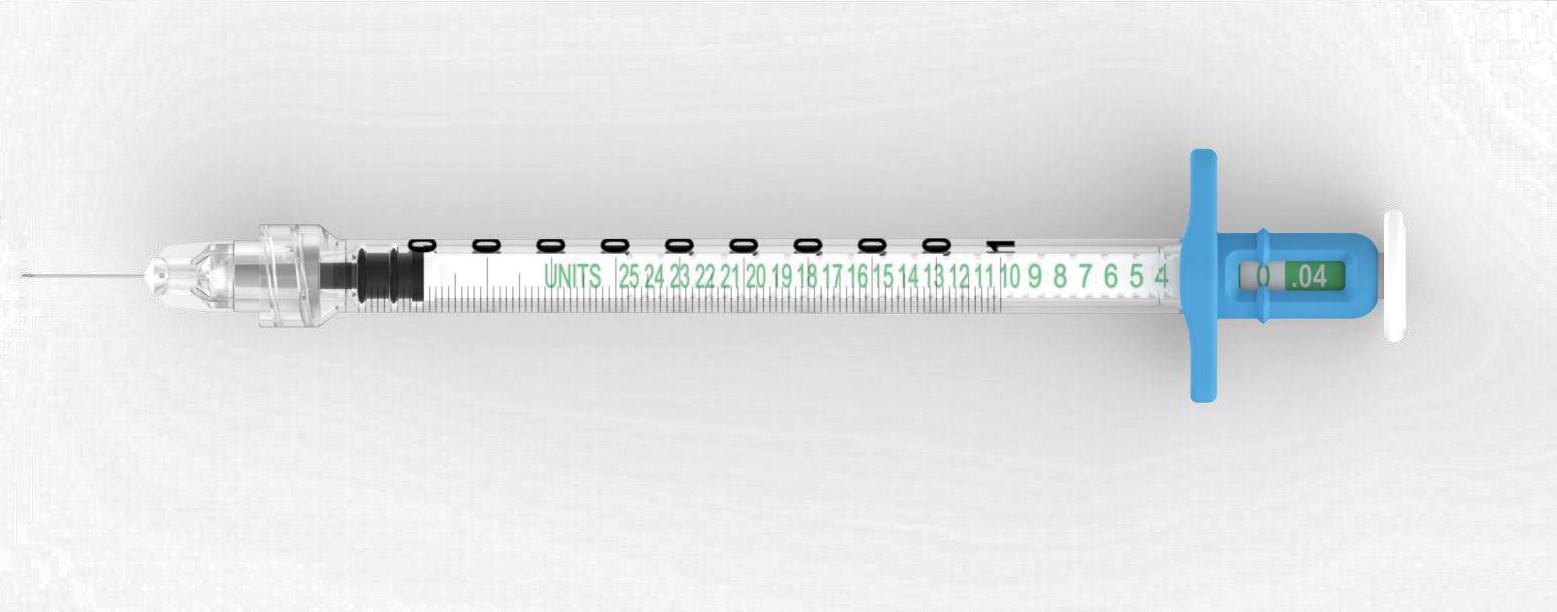
Figure 1: The 3Dose botulinum toxin syringe.

Figure 2: Contracted platysma, ideal for BoNTA treatment.
Conclusion
The clinician is advised to maintain a current and accurate awareness of the anatomy of the lower face, an appreciation of the age-related changes, as well as advances in the off-label indications of BoNTA, to deliver safe and effective treatments. In addition, the use of facial aesthetic scales are a useful consultation tool to discuss expected degree(s) of improvement with the individual. The clinician is able to enhance the accuracy of treatment outcome through utilising injection delivery systems, such as the 3Dose botulinum toxin syringe, which have been shown to enhance the precision of targeted product placement, and thus minimise the risk of complications when treating the lower face with BoNTA.
References
1. Carruthers JDA, Glogau RG, Blitzer A. Advances in facial rejuvenation: botulinum toxin type a, hyaluronic acid dermal fillers, and combination therapies-concensus recommendations. Plast Reconstr Surg 2008;121(5):5s-30s.
2. Geister TL, Gurk BB, Rzany B, et al. Validated assessment scale for platysmal bands. Dermatological Surgery 2013;39:1217-25.
3. Mendelson B, Wong CH. Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesth Plast Surg 2012;36:753-60.
4. Shaw RB, Katzel EB, Koltz PF, et al. Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg 2011;127(1):374-83.
5. Yang HM, Lee JG, Hu KS, et al. New anatomical insights on the course and branching patterns of the facial artery: clinical implications of injectable treatments to the nasolabial fold and nasojugal groove. Plast Reconstr Surg 2014;133(5):1077-82.
6. Gierloff M, Stöhring C, Buder T, Wiltfang J. The subcutaneous fat compartments in relation to aesthetically important facial folds and rhytides. Journal of Plastic, Reconstructive & Aesthetic Surgery 2012;65:1292-7.
7. Kim BW, Park GH, Yun WJ, et al. Adverse events associated with botulinum toxin injection: a multidepartment, retrospective study of 5310 treatments administered to 1819 patients. Journal of Dermatological Treatment 2013;64:1471-753.
8. Cavallini M, Cirillo P, Fundaro SP, et al. Safety of botulinum toxin A in aesthetic treatments: a systematic review of clinical studies. Dermatological Surgery 2014;40:525-36.
9. Xie Y, Zhou J, Li H, et al. Classification of masseter hypertrophy for tailored botulinum toxin type A treatment. Plast Reconstr Surg 2014;34(2):209e-218e.
10. Sinnatamby CS: Last’s Anatomy Regional and Applied. 11th Edition. Churchill Livingstone; 2006.
11. Choi YJ, Kim JS, Gil YC, et al. Anatomical considerations regarding the location and boundary of the depressor anguli oris muscle with reference to botulinum toxin injection. Plast Reconstr Surg 2014;134(5):917-21.
12. Shim KS, Hu KS, Kwak HH, et al. An anatomical study of the insertion of the zygomaticus major muscle in humans focused on the muscle arrangement at the corner of the mouth. Plast Reconstr Surg 2008;121(2):466-73.
13. Ascher B, Talarico S, Cassuto D, et al. International concensus recommendations on the aesthetic usage of botulinum toxin type A (Speywood Unit)-part II: wrinkles on the middle and lower face, neck and chest. Journal of the European Academy of Dermatology and Venereology 2010;24:1285-95.
14. Shadfar S, Perkins SW. Anatomy and physiology of aging neck. Facial Plast Surg Clinic N Am 2014;22:161-70. 15. Wu WTL. Microbotox of the lower face and neck: evolution of a personal technique and its clinical effects. Plast Reconstr Surg 2015;136(5s):92s-100s.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


