
Laser is an acronym for Light Amplification by Stimulated Emission of Radiation. Lasers have revolutionised the treatment of many skin conditions and are being used both in terms of a medical and an aesthetic context. Laser technology has been advancing and the number of laser applications in relation to the skin has increased significantly.
Lasers produce a beam of light of a specific wavelength (monochromatic). However, for a laser to have an effect the radiation, it has to be absorbed and then converted to heat. It therefore requires a chromophore (target). What makes the skin so susceptible to laser treatment is that it contains several chromophores. These chromophores are predominantly haemoglobin, melanin, water and foreign bodies.
The chromophore haemoglobin will selectively absorb light at 595nm (if using a pulsed dye laser) and the heat generated will potentially destroy the blood vessel. However, based on the theory by Anderson and Parrish of selective photothermolysis [1], if the pulse duration is short enough, the heat tends to be confined to the vessel and does not dissipate to the surrounding skin therefore producing selective damage to the vessel but leaving the rest of the skin intact.
Each chromophore in the skin absorbs light of a different wavelength and this explains why several different lasers are required to treat the full range of conditions involving the skin although there are machines which incorporate a number of lasers of different wavelengths.
In view of this, a logical way of understanding which lasers to use in the skin is to consider the wavelength of the laser, appreciate which chromophore absorbs light at this wavelength and then the clinical applications become clearer.
Vascular lasers
The vascular laser used most often in dermatology is the pulsed dye laser (PDL) with a wavelength of 595nm [2]. The initial use of the vascular lasers was in the treatment of port wine stains and is the treatment of choice for this condition (Figure 1). Other lasers such as the potassium titanyl phosphate (KTP) laser (532nm) and neodymium:yttrium-aluminium-garnet (Nd:YAG) laser (1064nm) also are used in vascular lesions and there are lasers which combine the use of the pulsed dye laser and Nd:YAG laser which may allow treatment of more complex vascular lesions.
The aim in children with port wine stains is to treat them as soon as possible with a view to trying to improve the port wine stain significantly prior to the child entering school.
Vascular lasers have led to a significant advance in the treatment of telangiectatic rosacea where patients complain of flushing and occasionally of a burning sensation of their skin related to vascular instability. By removing the superficial vessels this cosmetically reduces the redness as well as improving the symptoms of flushing or a burning sensation. The efficacy and safety profile of PDL in the treatment of erythematotelangiectatic rosacea are well established [3,4].
Rosacea can be a socially stigmatising disease since facial flushing and skin changes can be mistakenly attributed to alcohol abuse [5]. Many individuals seek treatment due to this misconception. As the condition is easily dealt with by lasers, this is a common aesthetic application for these types of lasers (Figure 2).

Figure 1: Port wine stain pre-treatment.
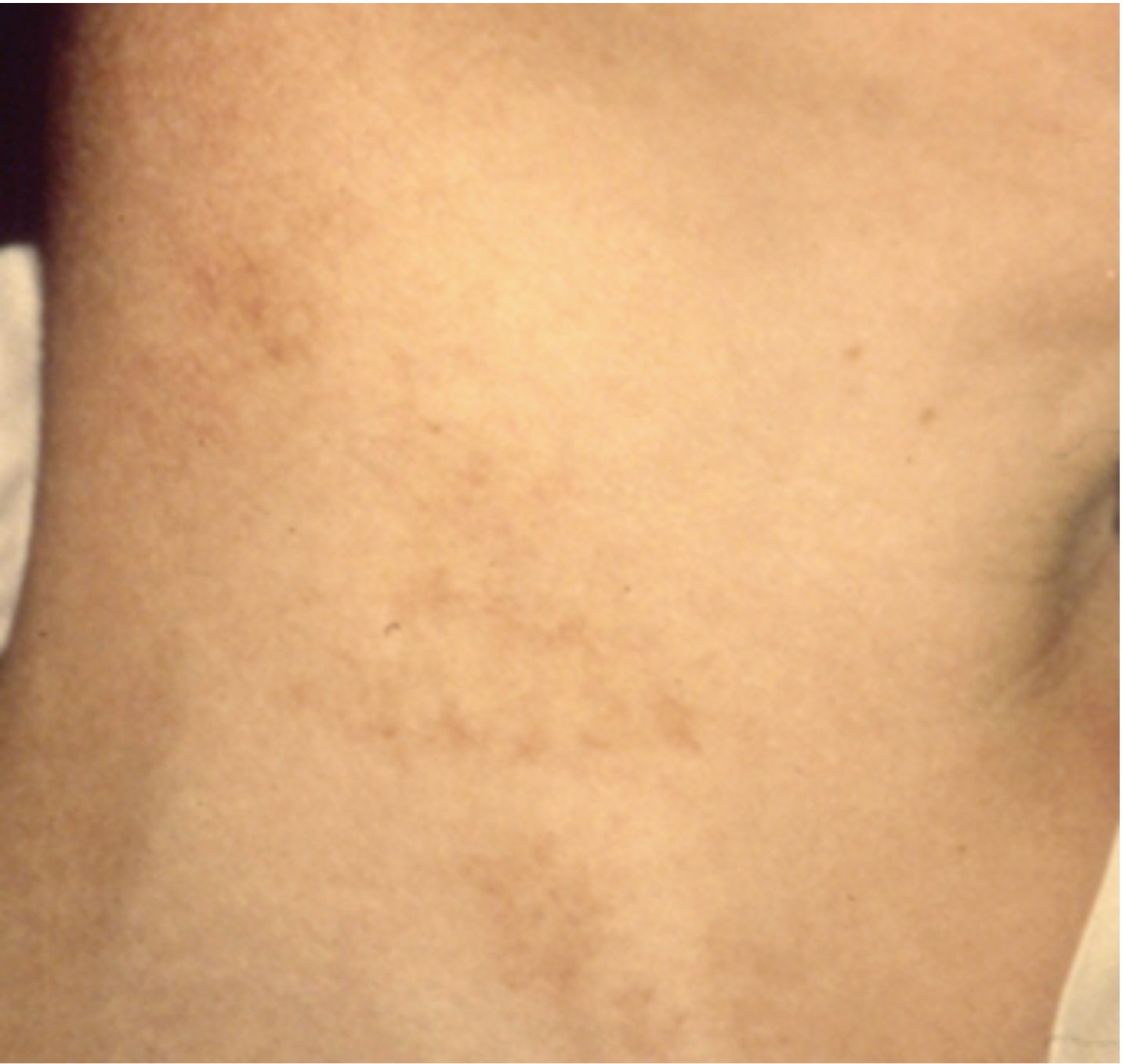
Figure 1: Post-treatment.
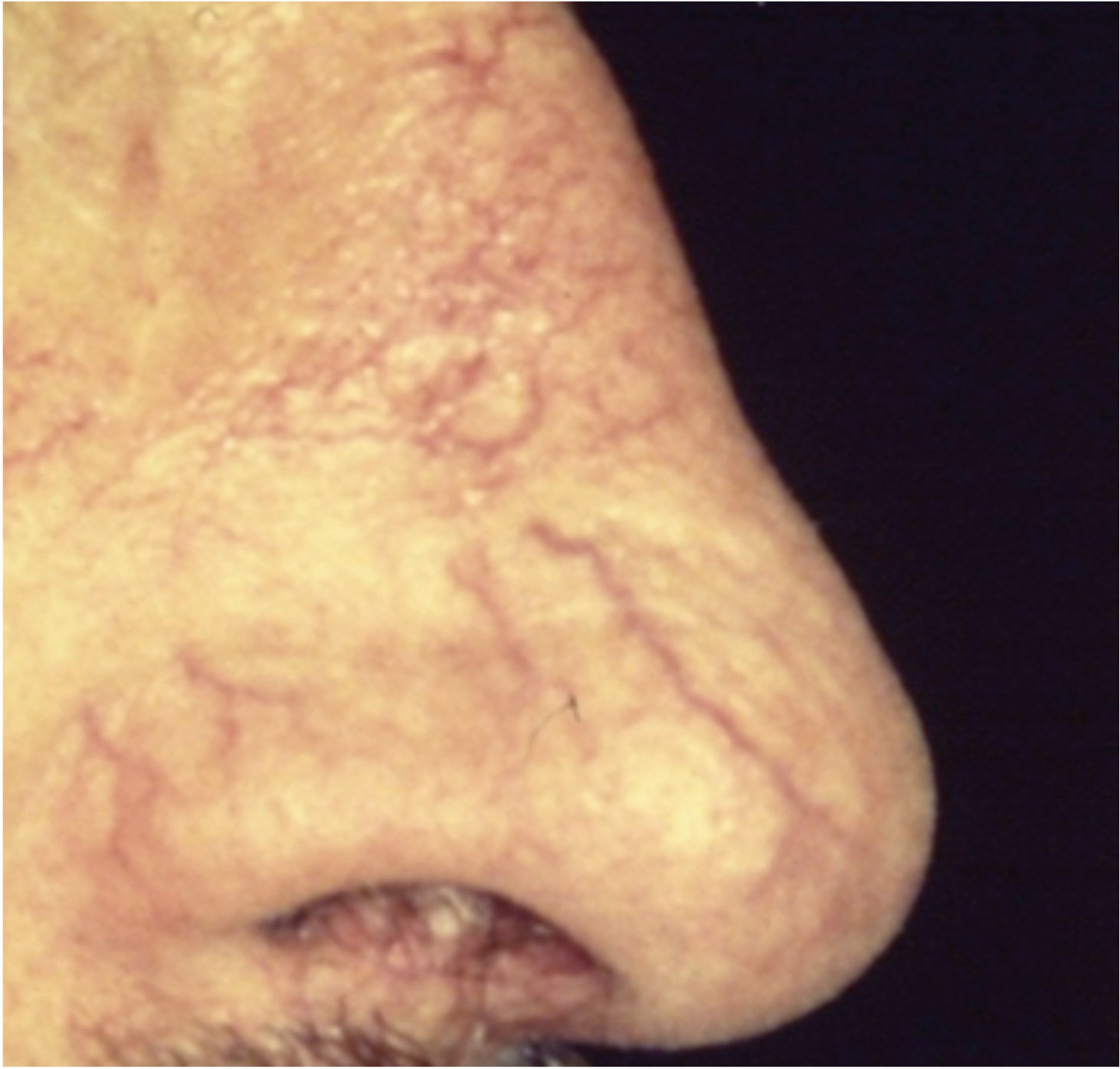
Figure 2: Telangiectasia pre-treatment.
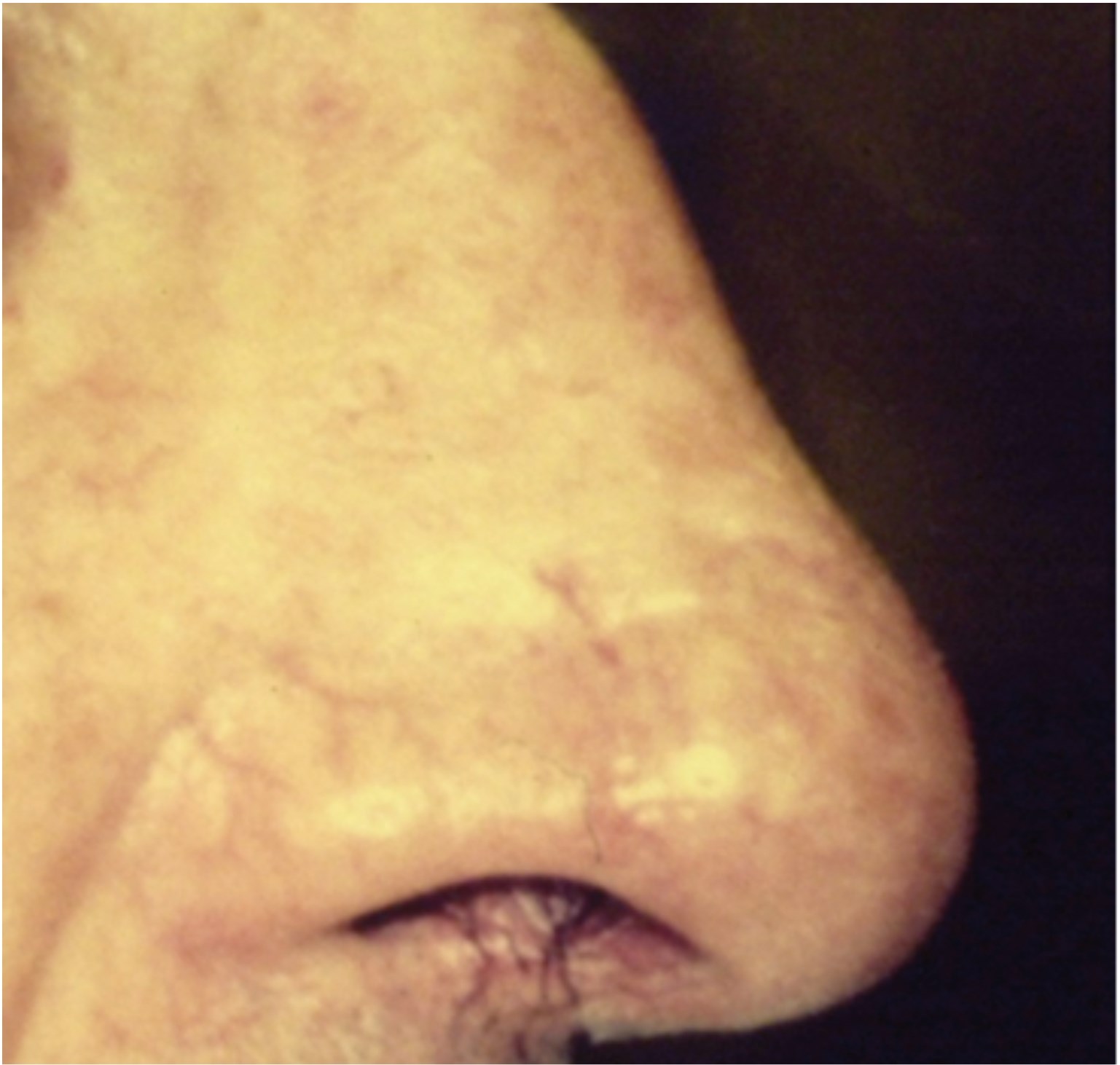
Figure 2: Post-treatment.
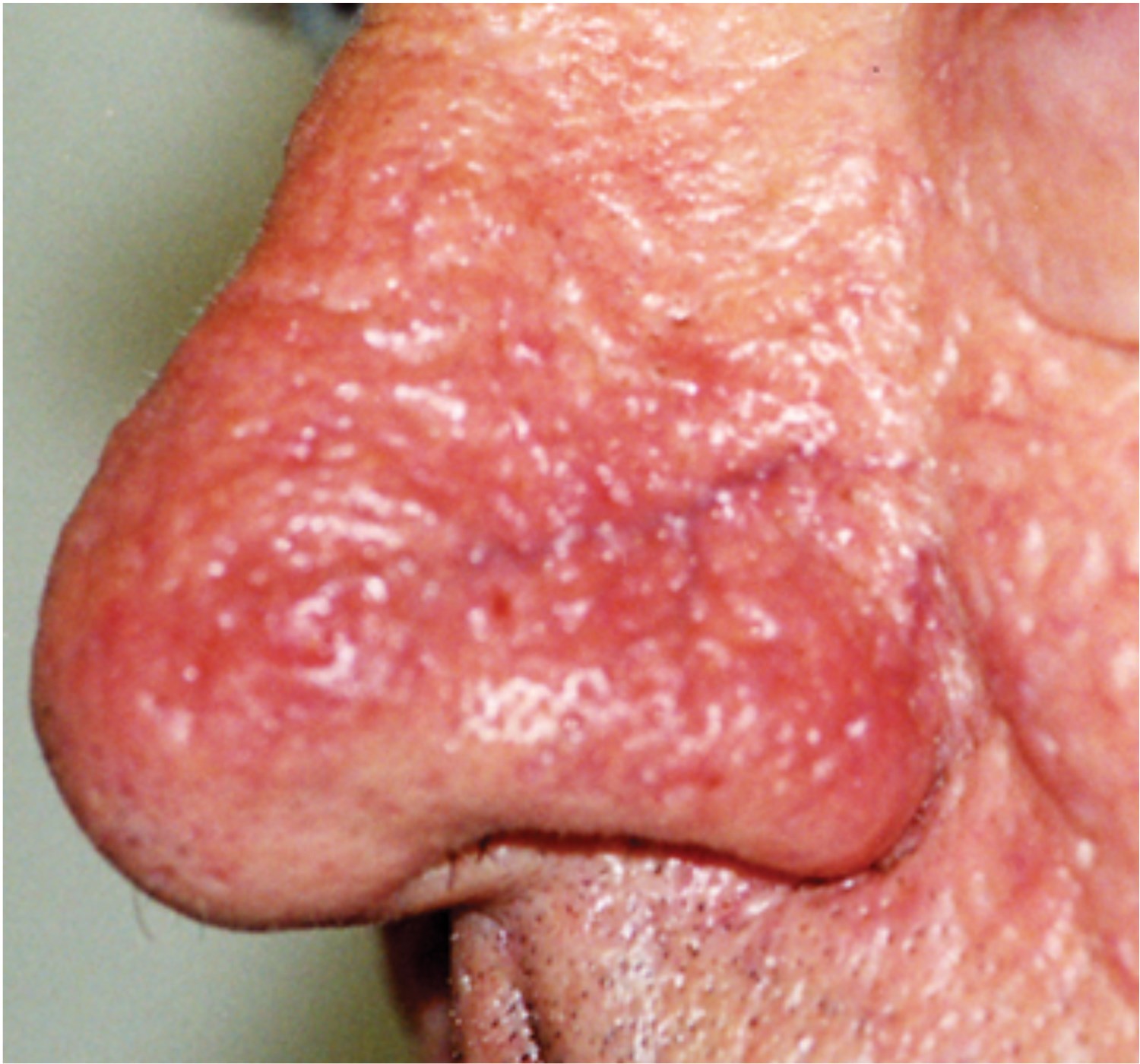
Figure 2: Telangiectasia pre-treatment.
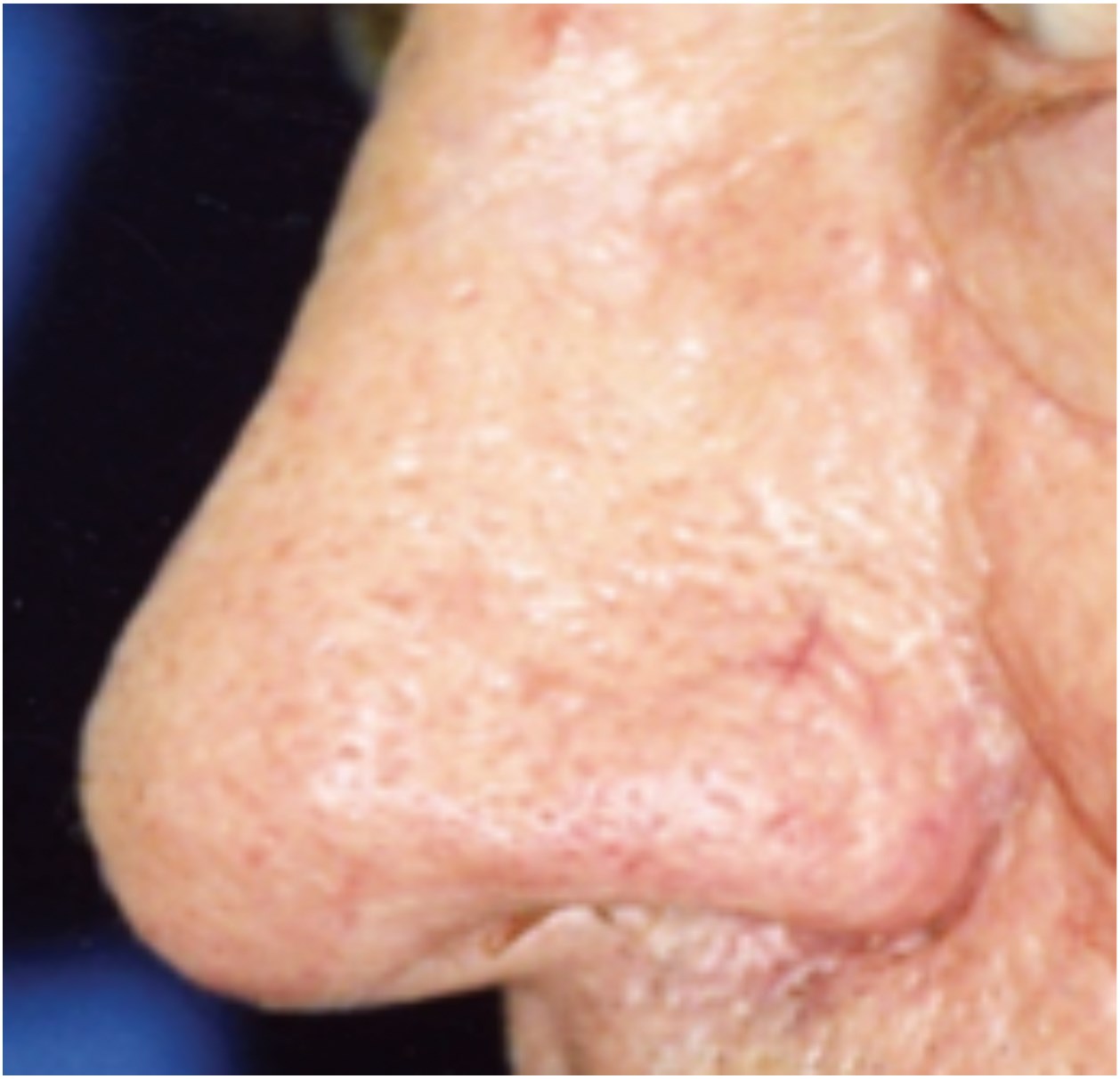
Figure 2: Post-treatment
Lasers for pigmentation and tattoos
The lasers used predominantly for pigmentation and the treatment of tattoos are the Q-switched Nd:YAG laser at a wavelength of 1064 or 532nm or the Alexandrite laser at 755nm. These lasers tend to target predominantly melanin or are absorbed by the tattoo pigment.
Medical conditions such as café au lait macules on the face and other rarer conditions such as naevi of ota are successfully treated. In terms of congenital melanocytic naevi, although one can reduce the pigmentation there is often a high risk of recurrence and there remains some concern as to whether laser treatment of these moles influences the risk of neoplasia.
Aesthetically photodamage, where lentigines are present, often responds well to the Nd:YAG laser. However, it is important that anyone undertaking treatment of this type of lesion must have a good understanding of the diagnosis and management of pigmented lesions.
In terms of tattoo removal, blue and black tattoos respond best to treatment; fortunately most amateur tattoos are this colour. Professional multicoloured tattoos take a significant increase in the number of treatments required. Green tattoos continue to require extensive treatment and have proved to be resistant.
However, a new generation of lasers known as picosecond lasers have recently been developed which are able to treat tattoos that proved resistant in the past [6].
Laser hair removal
One of the most common uses of lasers in the aesthetic industry is the removal of unwanted hair. The main lasers being used in this area are the Alexandrite laser, Diode laser (810nm) and long pulsed Nd:YAG laser(1064nm) in darker skins.
The aim is that light is absorbed by the melanin in the hair follicle with a view to trying to destroy the hair follicle. This has led to individuals having periods where their hair growth stops or reduces significantly but it does not tend to be permanent. The hairs that grow back are often thinner and have a lower density.
A course of six to eight treatments is initially required due the hairs present being in different cycles of anagen and telogen. Patients have a high level of satisfaction with this treatment [7].
Once clear, ‘top up’ treatments are generally required to maintain clearance. This has revolutionised the treatment of hirsutism for many women, particularly those with polycystic ovarian syndrome. However, the majority of women requesting treatment for hirsutism will not have an underlying medical condition.
Other medical conditions, such as the treatment of pilonidal sinuses, have been improved by removing the hair from the natal cleft [9]. Another clinical application is in individuals who have had amputations, particularly below the knee, who can get irritation on the stump due to hair growth and folliculitis. This can be improved by laser hair removal.

Figure 3: Photo ageing pre-treatment.

Figure 3: Post-treatment.

Figure 4: Acne scarring pre-treatment.
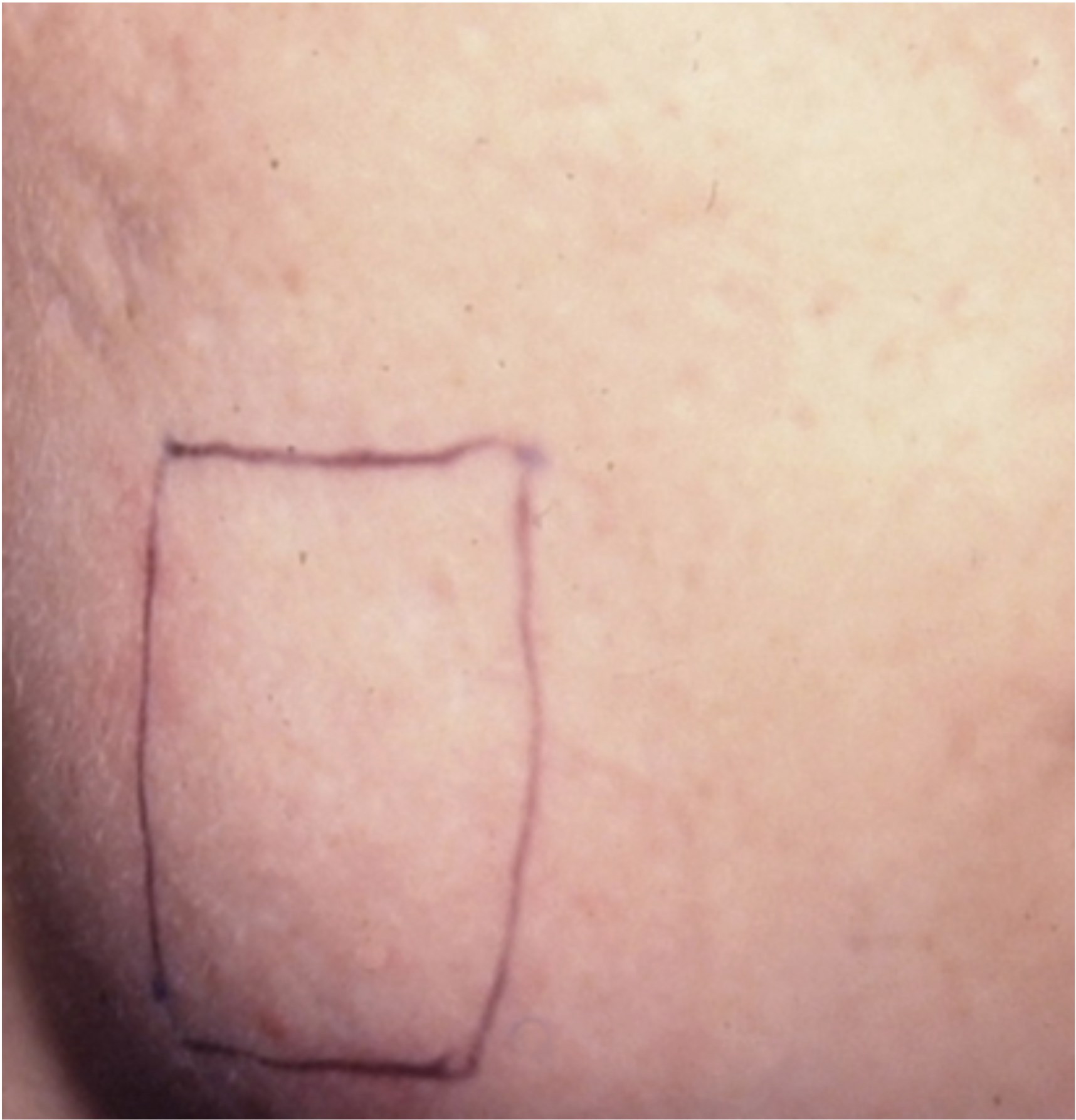
Figure 4: Post-treatment.
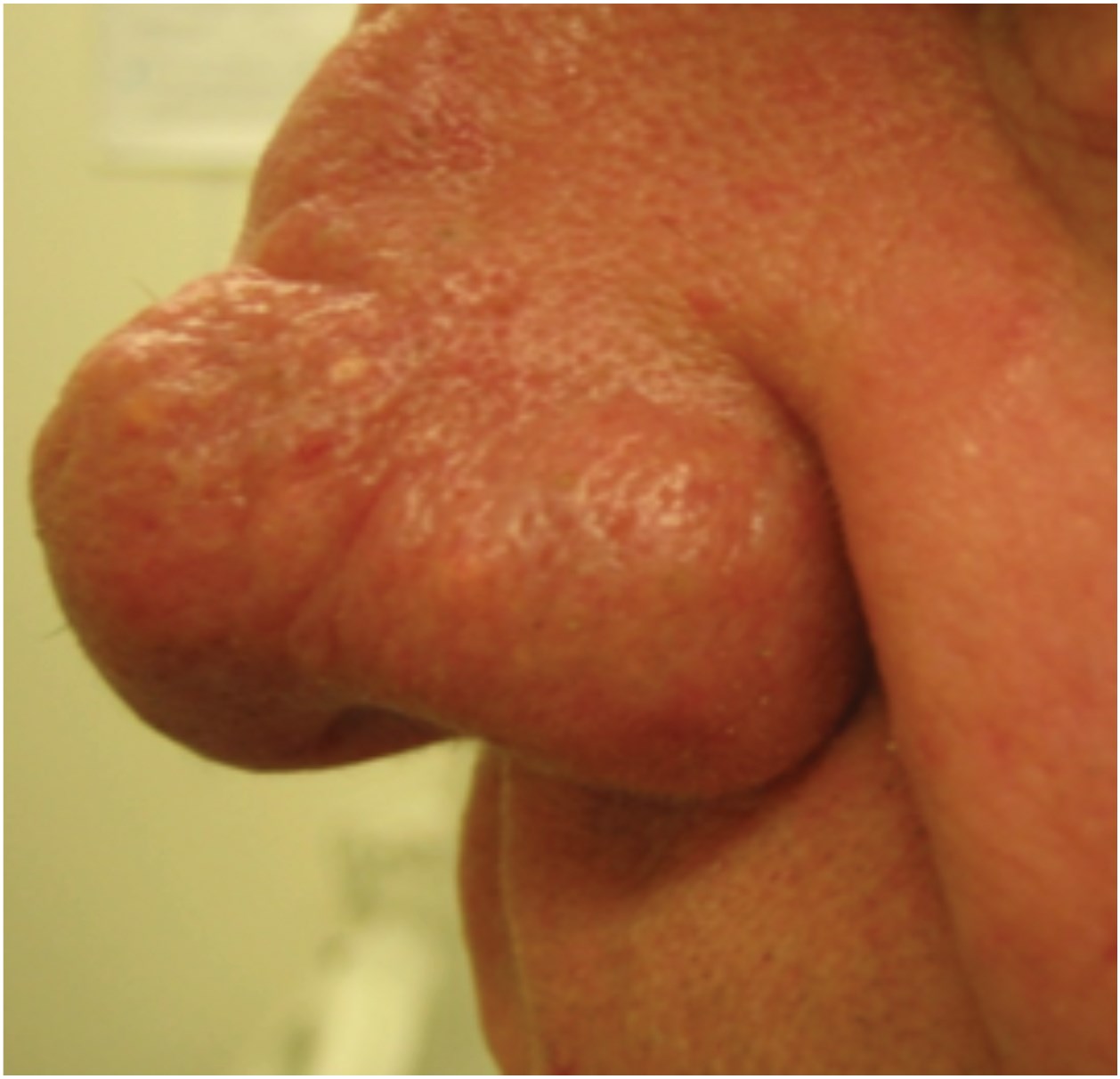
Figure 5: Rhinophyma pre-treatment.
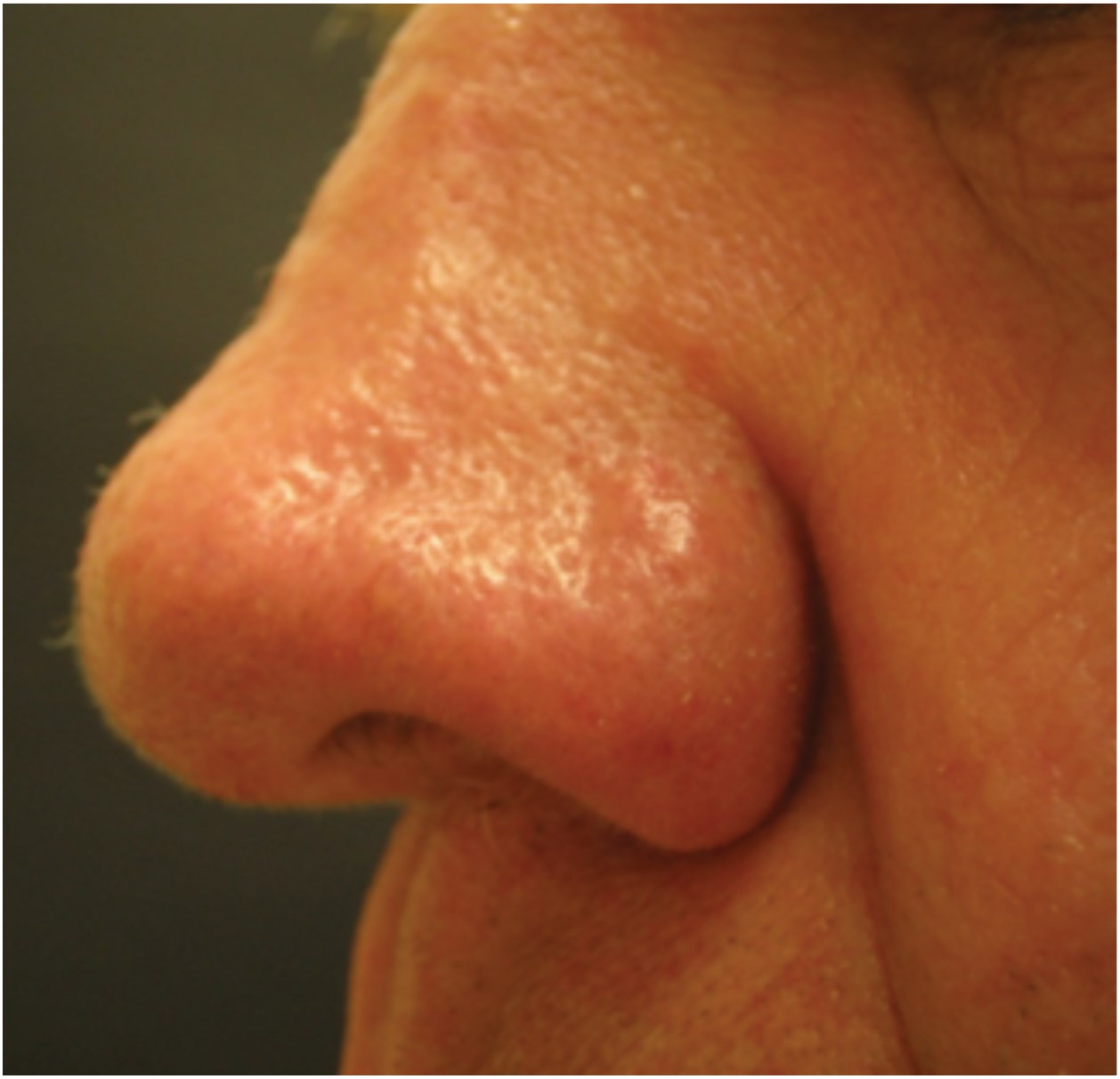
Figure 5: Post-treatment.
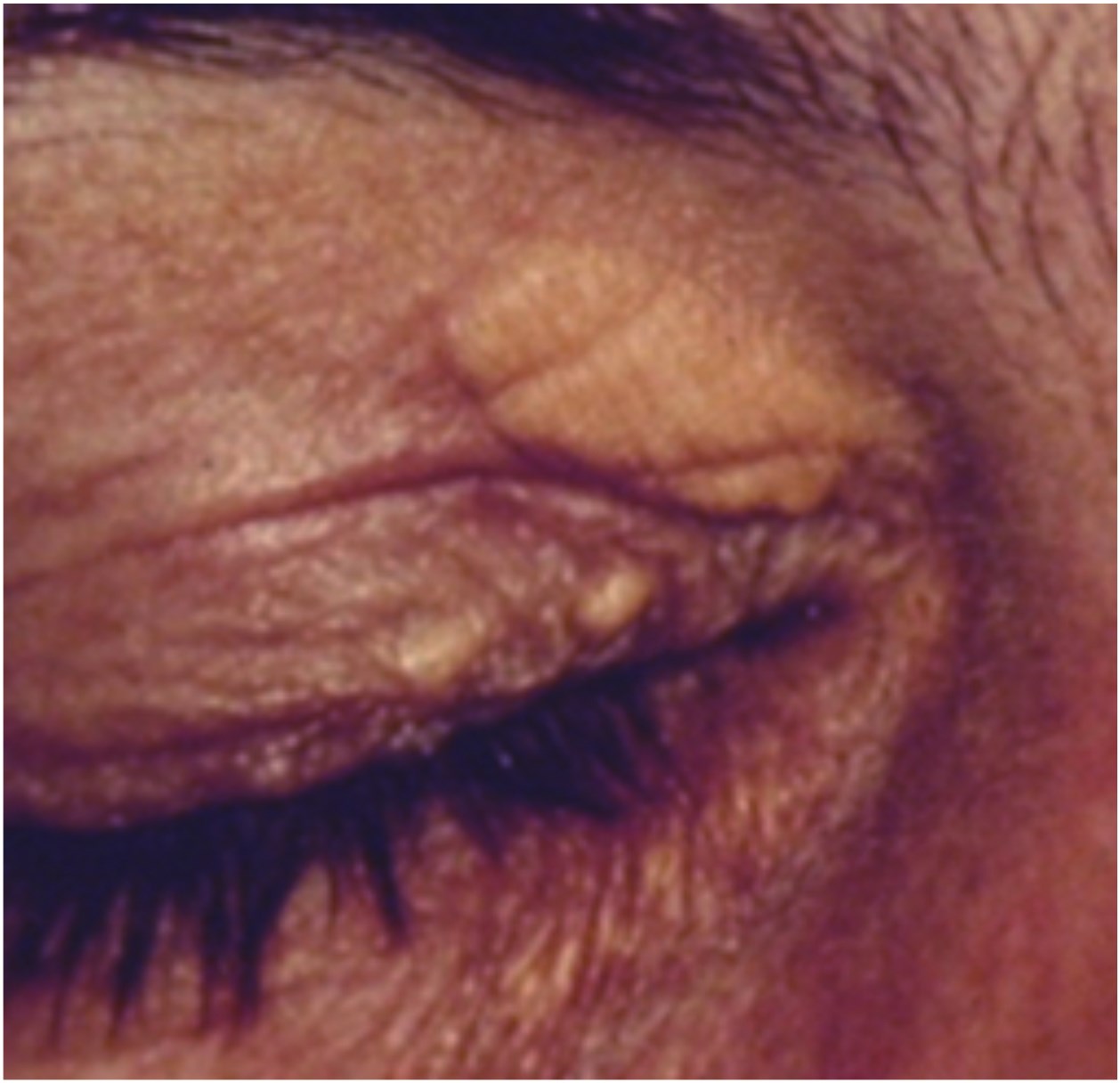
Figure 6: Xanthelasma pre-treatment.
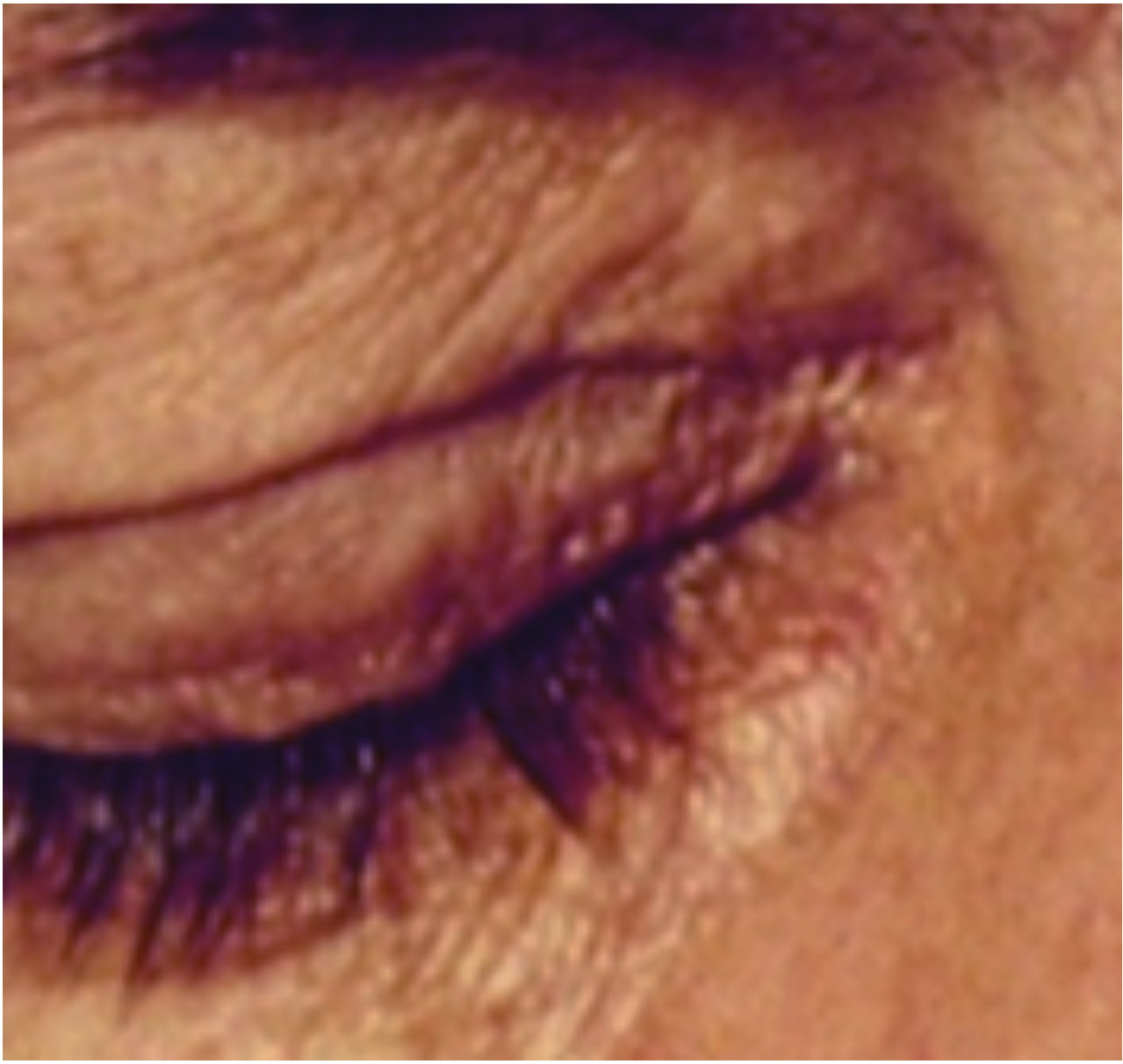
Figure 6: Post-treatment.
Ablative lasers
Ablative lasers were developed based on wavelengths that are absorbed by water. This allowed precise removal of the layers of the skin.
Continuous wave carbon dioxide lasers were initially used for laser resurfacing the skin which meant removing the skin layer by layer with a view to allowing the growth of new smoother, more evenly toned skin. However, these lasers still caused significant thermal damage with a high risk of scarring.
To reduce the thermal damage that occurred in the skin tissue pulsed carbon dioxide (CO²) (10600nm) laser systems were developed. These removed layers of skin in a more controlled manner. The Erbium YAG laser (2940nm) was also developed and its overall efficacy was comparable to the pulse and scanned CO² laser techniques. Both of these laser systems were described as ‘ablative lasers’ as they targeted the skin from the epidermis to the dermis.
It was noted that significant shrinkage of tissue during resurfacing took place. This shrinkage of tissue, indicating heat-induced collagen shrinkage, was thought to account for the smoother, tighter appearance of the skin.
Rapid reconstitution of the epidermis from adjacent epidermal cells contrasts with healing after traditional resurfacing in which new epidermis is derived from cells that migrate from adnexal structures. A prolonged period of dermal neocollagenesis of up to at least six months follows [9].
The aesthetic applications of ablative lasers have expanded significantly. In particular photo-ageing leading to the development of lines and wrinkles particularly around the eyes and mouth can be treated. Skin texture can be improved significantly and lentigines removed (Figure 3).
Other applications
Ablative lasers have led to significant advances in the treatment of scarring particularly in relation to acne scarring [10]. Acne scarring can be a mixture of shallow fibrotic scars known as atrophic scars, deep ice-pick scars, rolling box scars and hypertrophic scarring.
Therefore, the treatment of acne scarring often requires different depths of ablation depending on the type of scarring one is dealing with (Figure 4). Ablative lasers have also been used in the treatment of surgical scars and burn scars.
Rhinophyma is a slowly progressive, disfiguring disorder of the nose which represents the end stage of acne rosacea. The cosmetic deformity is often the reason for patients to seek medical attention. Ablative lasers can be used for incisional surgery and have the advantage of non-contact with the skin, haemostasis, reduced postoperative pain and sealing of lymphatic channels.
The CO² laser provides a dry surgical field which allows the sculpting of the hypertrophic areas to be very effective, giving a very satisfactory cosmetic result (Figure 5). Neurofibromata can be ablated quickly and effectively allowing large numbers of nodules to be removed at one time. Xanthelasma is another condition which responds well to the precision of laser ablation (Figure 6).
Laser ablative resurfacing is considered the gold standard against which all other facial rejuvenating systems are compared.
Fractionated resurfacing
Newer modalities use the principles of fractional photothermolysis (FP) to create patterns of tiny microscopic wounds surrounded by undamaged tissue beneath the skin. These devices produce more modest results than traditional CO² lasers but with fewer side-effects and shorter recovery periods [11,12] but may need several treatments. Fractional technology has been applied to Erbium YAG lasers as well.
The fractionated component of the laser allows for a spatially precise, regular pattern of columns of tissue injury across the treated area, retaining the healing function of the epidermis. In theory these lasers provide the significant resurfacing capabilities of an ablative laser while retaining the reduced recovery time of a non-ablative laser. However, because the laser targets a fraction of the patient’s skin at a time, more treatments are required.
Laser resurfacing continues to be a useful technology and the decision whether to use a full ablative treatment versus a fractionated ablative treatment is often based on the recovery time and severity of the condition.
Even with fractionated technology there can be a risk of complications [13] such as infection, altered pigmentation, and scarring which emphasises the need for appropriate patient selection and training with all forms of lasers.
In summary, laser technology continues to improve and there is an increasing number of skin conditions amenable to laser surgery.
References
1. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science 1983;220:524-7.
2. Chen JK, Ghasri P, Aguilar G, et al. An overview of clinical and experimental treatment modalities for port wine stains. J Am Acad Dermatol 2012;67(2):289-304.
3. Jasim ZF, Woo WK, Handley JM. Long-pulsed (6-ms) pulsed dye laser treatment of rosacea-associated telangiectasia using subpurpuric clinical threshold. Dermatol Surg 2004;30:37-40.
4. Clark SM, Lanigan SW, Marks R. Laser treatment of erythema and telangiectasia associated with rosacea. Lasers Med Sci 2002;17:26-33.
5. Powell FC. Clinical Practice. Rosacea. NEJM 2005;352:793-803.
6. Brauer JA, Reddy KK, Anolik R, et al. Successful and rapid treatment of blue and green tattoo pigment with a novel picosecond laser. Arch Dermatol 2012;148(7):820-3.
7. Preston PW, Lanigan SW. Patient satisfaction with laser hair removal. J Cosmet Dermatol 2003;2(2):68-72.
8. Koch D, Pratsou P, Szczecinska W, et al. The diverse application of laser hair removal therapy: a tertiary laser unit’s experience with less common indications and a literature overview. Lasers Med Sci 2015;30(1):453-67.
9. Orringer JS, Kang S, Johnson TM, et al. Connective tissue remodeling induced by carbon dioxide laser resurfacing of photodamaged human skin. Arch Dermatol 2004;140(11):1326-32.
10. Hession MT, Graber EM. Atrophic acne scarring: a review of treatment options. J Clin Aesthet Dermatol 2015;8(1):50-8.
11. Serowka KL, Saedi N, Dover JS, Zachary CB. Fractionated ablative carbon dioxide laser for the treatment of rhinophyma. Lasers Surg Med 2014;46(1):8-12.
12. Preissig J, Hamilton K, Markus R. Current laser resurfacing technologies: a review that delves beneath the surface. Semin Plast Surg 2012;26(3):109-16.
13. Fife DJ, Fitzpatrick RE, Zachary CB. Complications of fractional CO² laser resurfacing: four cases. Lasers Surg Med 2009;41(3):179.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


