
3D printing was first developed in the 1980s, but it wasn’t until the early 2010s that the additive manufacturing or 3D printing technology advanced enough to become available to those outside of specialist laboratories.
3D printing has also begun to be used in the medical setting. In plastic and maxillofacial surgery, 3D printing has been used in the soft tissue reconstruction of Parry-Romberg syndrome [1], in the planning of surgeries, dental implants [2] and extensively in craniofacial reconstructions [3]. With the potential of 3D printers being realised and the involved costs decreasing, teams around the world are now starting to use 3D scanning and printing technology in the planning and execution of reconstructive surgery [4].
Whilst external companies offer services printing medical models from scans, keeping printing in-house should enable costs to be kept down. Therefore, the aim of this article is to examine the types of printing available and which would be best suited to printing models for use in reconstructive surgery.
“Which printer is needed is likely to be decided by the size of the object that is needed to be printed, how they can be sterilised for use in the theatre environment, and the cost that the purchasing department can afford”

Types of printer
There are three types of printing: fused deposition modelling (FDM), stereolithography (SLA or SL) and selective laser sintering (SLS).
Fused deposition modelling
FDM was developed in the late 1980s and uses a range of plastics. It works by extruding strings of polymer from a heated nozzle, laying the polymer string down in rows to form a three-dimensional structure. Examples of FDM printers include Makerbot®, Stratasys® uPrint, and Stratasys Mojo.
Its ability to print with a range of plastics means that FDM printers have multiple uses. They are relatively inexpensive machines to purchase, and also have lower consumables. Setting up and running costs are therefore low for this type of printer.
However, its method of printing – strings of plastic layered on top of each other – makes certain shapes difficult to print. Extensive supports are therefore required in order to print complex objects, and these supports need to be removed post-printing. In addition, only rigid plastics can be used and it is difficult to print porous models.
Stereolithography
SLA printers, on the other hand, use photopolymers. Printers include Stratasys Objet24 and Objet30 Pro, and Formlabs Form 1+.
SLA printers work by employing a vat of liquid curable photopolymer (‘resin’), which is then hardened by a beam of an UV laser light. These printers are much more accurate than FDM, and don’t need to use extensive supports (although easily removable gel supports are often used). It is possible to use flexible materials with SLA printers, and it is possible to print porous and mesh-like models.
However, the SLA printers have higher consumables and the materials are not very durable. Durability of the materials may not be an issue however, depending on what is being printed.
Selective laser sintering
SLS printers are the best (and the most expensive) technology, an example of which is the ProX® SLS 500 from 3D systems. They use laser as the power source to sinter powdered material (granules) to make a solid model. It is the most accurate of the three printer types and there is no need for external supports during the printing process. SLS printers produce objects with a very smooth finish and have the potential to use different materials in a single printed object. Unlike the other printers, they are suitable for the creation of large objects.
However, as SLS printers are much more expensive than the FDM and SLA technologies, this type of printer would be the least cost-effective for small scale productions. As this printer would not be cost-effective for most in-house healthcare printing needs, we looked further into the FDM and SLA technologies.
Other considerations
Apart from the method of printing there are a few more questions that need to be considered when choosing a printer. These are:
- Which material does the object need to be printed in? Options include plastics, resins and rubbers.
- How large does the printer need to be able to print?
- What level of accuracy is needed from the print?
- Does the object need to be sterilised?
- What is the cost?
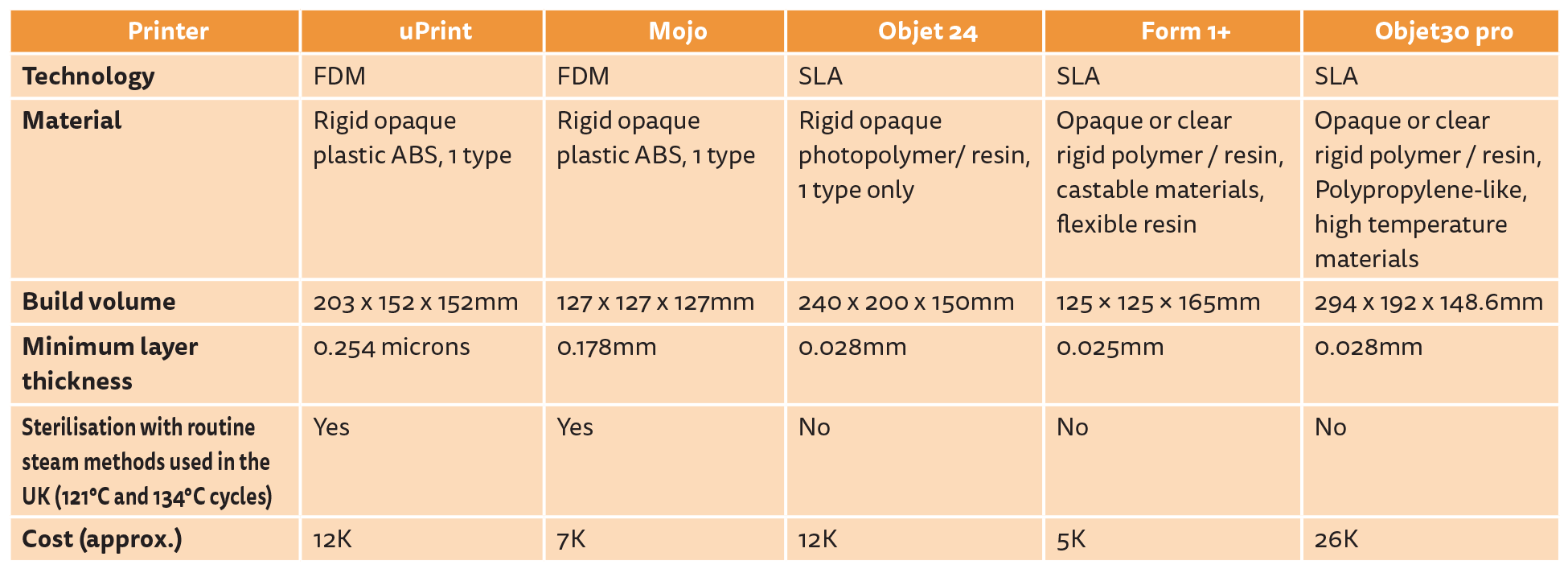
We made a comparison from manufacturer data of the above five points between five different printers (two FDM and three SLA), the results of which are shown in the table above (data was accurate at the time of compiling the article and may have changed since).
After consideration of the above, the Stratasys range of 3D printers (uPrint, Mojo, Objet 24, Objet30 pro) appear to be well-suited to general entry-level needs, although they do offer some very advanced solutions. The Objet24 SLA printer is an entry-level printer that would allow accurate printing in rigid plastics.
Using the same principle as the Objet and Eden printers, the Form 1+ printer offers UV-cured printing for less than £5000, and also offers a resin for flexible prints. However, this is a much smaller company and therefore it is important to confirm that they will be able to offer the same level of technical support as a larger, more established company in case of any problems. Additionally, its ability to only print 125x125x165mm models in comparison to 240x200x150mm from Objet24 may make it unsuitable as it would limit the scope of projects.
When investing in a 3D printer, it is important to think not only of the immediate uses, but also of potential future uses. For example, if having the possibility to print in a rubber-like material is important, then a printer from a higher tier such as the Eden printer from Objet would be needed. However, a printer with higher capabilities is more expensive, and may be too expensive for an initial purchase.
Conclusion
There are many three-dimensional printers available, printing using a variety of techniques and in a variety of materials. Ultimately, which printer is needed is likely to be decided by the size of the object that is needed to be printed, how they can be sterilised for use in the theatre environment, and the cost that the purchasing department can afford.
References
1. Chai G, Tan A, Yao CA, et al. Treating Parry-Romberg syndrome using three-dimensional scanning and printing and the anterolateral thigh dermal adipofascial flap. J Craniofac Surg 2015;26(6):1826-9.
2. Yun PY. The application of three-dimensional printing techniques in the field of oral and maxillofacial surgery. J Korean Assoc Oral Maxillofac Surg 2015;41(4):169-70.
3. Choi JW, Kim N. Clinical application of three-dimensional printing technology in craniofacial plastic surgery. Arch Plast Surg 2015;42(3):267-77.
4. Li Y, Jiang Y, Ye B, et al. Treatment of dentofacial deformities secondary to osteochondroma of the mandibular condyle using virtual surgical planning and 3-dimensional printed surgical templates. J Oral Maxillofac Surg 2016;74(2):349-68.
Further information:
Please see the manufacturer’s websites for more information:
www.stratasys.com
http://formlabs.com
www.3dsystems.com
Declaration of competing interests: None declared.
TAKE HOME MESSAGE
-
3D printing is becoming increasingly used in surgical planning and in reconstruction.
-
There are three types of 3D printers available: fused deposition modelling (FDM), stereolithography (SLA or SL) and selective laser sintering (SLS).
-
FDM printers lay the polymer string down in rows to form a three-dimensional structure.
-
SLA printers use liquid resin that is hardened by a beam of an UV laser light.
-
SLS printers use laser to sinter granules to make a solid model.
-
When choosing a printer, the important questions are whether the printer meets the department’s needs in terms of material, size, accuracy and sterilisation.
COMMENTS ARE WELCOME


