
Liposculpture involving fat transfer to the buttocks (‘Brazilian butt lift’) has experienced a dramatic increase in demand in recent years. Popular tabloid celebrities have fuelled the demand for this procedure, resulting in large numbers of patients requesting buttock enhancement surgery. Fat grafting is highly successful in the gluteal area. A large surface area acting as the recipient bed enables the transfer of large quantities of fat graft with excellent results.
Low-pressure tumescent liposuction, power assisted liposuction and ultrasound assisted liposuction are common fat harvesting techniques [1-4]. In recent years, Water Jetstream liposuction has gained popularity as an excellent method for large volume fat grafting procedures [5]. The following report presents our experience of water jetstream liposuction for buttock fat grafting.
Patient selection
Liposculpture with fat transfer to the buttocks is an operation that will benefit the vast majority of female patients. Most individuals have extra diet resistant fat deposits in the lower back, abdominal or saddlebag area, which they are more than happy to exchange for firmer and more projecting buttocks. Generally, we differentiate between primary and secondary buttock fat transfer procedures. In primary buttock fat transfer, patients are primarily interested in enhancing and augmenting the buttocks. Fat reduction in the donor site is only a secondary concern to these patients. Patients of the ‘primary’ augmentation group sometimes ask for very large transfer volumes (Figures 1 and 2).
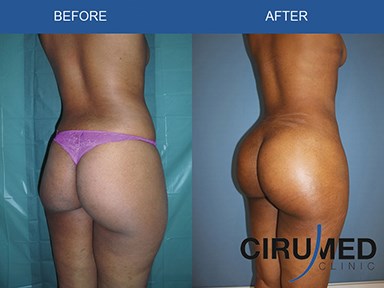

Figure 1: Water Jetstream assisted liposculpture (grafted volume approx. 1000cc per buttock).


Figure 2: Buttock reshaping with water jetstream fat transfer (900cc graft per buttock).
In ‘secondary’ augmentation cases, patients are primarily concerned about their ‘problem zone’ fat deposits. They are generally not overly concerned with their buttocks. However, in many of these patients the addition of fat transfer to enhance the overall outcome can dramatically improve the result (Figure 3).


Figure 3: 750cc per side grafted volume, note aesthetic
effect of volume reshifting from ‘love handles’ to buttocks.
When assessing a patient for fat transfer, one needs to differentiate between the four main buttock shapes, namely A, C, H and V-shape. The differences between these shapes are often somewhat blurred, and one may easily find characteristics of two different shapes in the same patient. In our experience, we have noted that individual patients’ preferences can vary dramatically; some patients ask for extensive widening of their frame whilst others (A-shape) look for maximum central roundness (C-shape).
Fat harvesting techniques
The majority of Brazilian butt lift surgeries in our department are performed using local anaesthetic with twilight sedation. Water jetstream liposuction is relatively painless, fairly stress-free and has very little blood loss. We believe it is impossible to draw an exact comparison between harvesting speeds, since different textures of fat in each individual patient in itself will cause important variances in extraction times. However, in a retrospective comparison against our mean harvesting time of equivalent amounts of fat, we found that water-jetstream liposuction is around 20% faster at obtaining fat grafts.
For transfer volumes of up to 2000cc, water jetstream assisted fat transfer procedures are handled as a day-case. Typical fat harvest areas are the abdomen, the lower back and the flanks (‘love handles’). For extraction of fat, we use BodyJet EVO technology, which provides a specific fat transfer mode, automatically adjusting the suction pressure to a maximum of 350-400mmHg. The original lipocollector protocol does not require further processing of the grafts [5]. The BodyJet system can be connected to a so-called lipocollector system, which essentially acts as a filter, producing a ready to inject graft.
We have refined our procedures to further purify the part of the graft that is designated to be placed in the more superficial layers of the body where there is less muscle tissue. These areas are more challenging with view to good graft take. The less vascularisation of the recipient bed, the more difficult it is to get good graft take. Superficial implantation accounts for approximately 30% of grafted fat. This area is of particular importance because superficial grafting is key to the final shape, much more than the deep grafting into the muscle.
To enhance graft survival in this area, we have refined our methods with further purification of fat using hand-spun centrifugation. Overall the yield from the above technique of fat-harvesting compares favourably to conventional fat harvesting processes with low pressure tumescent liposuction. Roberts et al. reported a yield of 50% of the total amount (for example, to obtain 800cc of purified graft, it was necessary to gain 1600cc of fat). With Water jetstream liposuction we gained an average of 80% of graftable fat from the total extracted amount, which is a significantly better performance compared to tumescent liposuction.
Fat grafting
Fat grafting is carried out in layers, placing grafts onto intramuscular and subcutaneous surfaces. The subcutaneous injection is especially important to achieve the desired roundness. Since this layer is not very well vascularised, fat transplantation here is technically challenging [3,6]. Fan-shaped microtunneling with 17G cannulas can be time-consuming and presents many difficulties, but excellent shaping results are achieved as a result of superficial grafting in the gluteal region using this method.
Anaesthesia and aftercare
In the majority of cases, we perform the procedure under sedation. The pulsed water jetstream liposuction as such is not too painful since separation of fat lobules from fibrous tissue is stress-free and there is continuous irrigation-suction with local anaesthetic.
All patients were ASA I, and for transfer volumes up to 2000cc the use of water jetstream was combined with deep intravenous sedation. For transfer volumes exceeding 2000cc and where patients specifically requested, general anaesthesia was used. At the end of the procedure, kinesiotaping was applied to the donor areas. We have found this to be helpful in reducing postoperative bruising and swelling. At the same time, the tapes increase patient comfort. Kinesiotaping is maintained for a total of 14 days.
Pressure garments are worn for six weeks. We instruct patients not to sit at all for the first 14 days postoperatively and to sleep in a prone position. For a further 14 days, we recommend to sit as little as possible. We do not find it necessary to restrict sitting beyond four weeks postoperatively.
Results
We have reviewed 336 cases of buttock augmentation with the amended water jetstream procedure (with added cell purification). To monitor fat stability, we usually take a photograph intraoperatively to document the volume before any resorption takes place. When comparing this with a photograph of the patient three months after the procedure, we usually find a very similar volume, corresponding to around 80-90% volume preservation.
However, if patients do not comply with strict no-sitting for the first two weeks, volume loss can occur. We have not observed any significant volume loss in patients compliant with postoperative instructions. Ninety-five percent of patients registered high levels of satisfaction with the outcome, and stated that they would do the procedure again.
Discussion
Fat grafting of the buttocks is a very flexible option for shaping the gluteal area. It compares favourably to implants regarding final shape, postoperative recovery and possible complication rate. With refined fat grafting procedures, it has become very rare for us to resort to implants (less than 10% of our gluteal augmentation patients have implants). Although fat transfer buttock augmentation is currently an extremely popular procedure, scientific literature dealing with it is still somewhat limited [2,5,7,8].
There is a broad consensus amongst surgeons reporting on this topic that the buttocks are especially receptive to fat transfer [2,3,5,7]. Intramuscular fat grafting to the gluteus muscle is generally believed to have excellent success rates. Power assisted liposuction, ultrasound and low pressure tumescent are frequently used techniques and all doctors sharing their experience believe that these specific methods all yield good results [1-4,9].
Water jetstream liposuction is a modern and relatively stress-free liposuction technique that enables surgeons to perform large volume fat grafts in a short amount of time. Its efficiency for fat transfer breast augmentation has been well established [5].
"...if patients do not comply with strict no-sitting for the first two weeks, volume loss can occur."
Conclusion
Water jetstream liposuction is a very valid option for surgeons with an interest in large volume fat transfer to the buttocks procedures. Our experience suggests that this technology will enhance the outcome of such operations. Some amendments of the original lipocollector procedure are recommended, especially for the more superficial lateral grafting.
References
1. Coleman SR. Long-term survival of fat transplants: controlled demonstrations. Aesthetic Plast Surg 1995;19:421-5.
2. Cardenas-Camarena L, Lacouture AM, Tobar-Losada A. Combined gluteoplasty: liposuction and lipoinjection. Plast Reconstr Surg 1999;104:1524-31.
3. Chajchir A, Besaquen I. Fat-graft injection for soft-tissue augmentation. Plast Reconstr Surg 1989;84:921-34.
4. Mendieta C: The Art of Gluteal Sculpting. Quality Medical Publishing Inc; 2011:149-2445.
5. Ueberreiter K, von Finckenstein JG, Cromme F, et al. BEAULI™ - eine neue Methode zur einfachen und zuverlässigen Fettzell-Transplantation (BEAULI™ - a new and easy method for large-volume fat grafts). Handchir Mikrochir Plast Chir 2010;42(6):379-85.
6. Chang KN. Surgical correction of post-liposuction contour irregularities. Plast Reconstr Surg 1994;94:126-36.
7. Pereira LH, Radwanski HN. Fat grafting of the buttocks and lower limbs. Aesthetic Plast Surg 1996;20:409-16.
8. Roberts TL 3rd, Toledo LS, Badin AZ. Augmentation of the buttocks by micro fat grafting.
Aesthet Surg J 2001;21(4):311-9.
9. Gasparotti M, Lewis CM, Toledo LS: Superficial liposculpture: manual of technique. New York: Springer-Verlag; 1996:83-9.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


