
This article has been verified for CPD. Click the button below to answer a few
short questions and download a form to be included in your CPD folder.

Minimally invasive cosmetic procedures, including lip augmentation using hyaluronic acid dermal fillers, are the most sought-after treatments according to recent American Society of Plastic Surgeons (ASPS) statistics, with those under 30 being the most common patient seeking lip augmentation [1].
The lips comprise a significant aesthetic unit contributing to the perception of youth and beauty, playing a key role in verbal and non-verbal communication, conveying facial expression and sensual attraction.
Knowledge of lips and perioral anatomy, combined with awareness of the morphological variations occurring on account of diversity such as age, gender and ethnicity, will assist us to implement strategies to achieve safer and more natural results.
Boundaries
When treating a particular facial region, it is important to recognise its boundaries. The perioral complex including lips is the area defined:
- Superiorly by the nasal bone
- Laterally by the cheeks, some authors may or not include the nasolabial folds
- Inferiorly by the labiomental crease, which is the anatomical boundary between the perioral area and chin
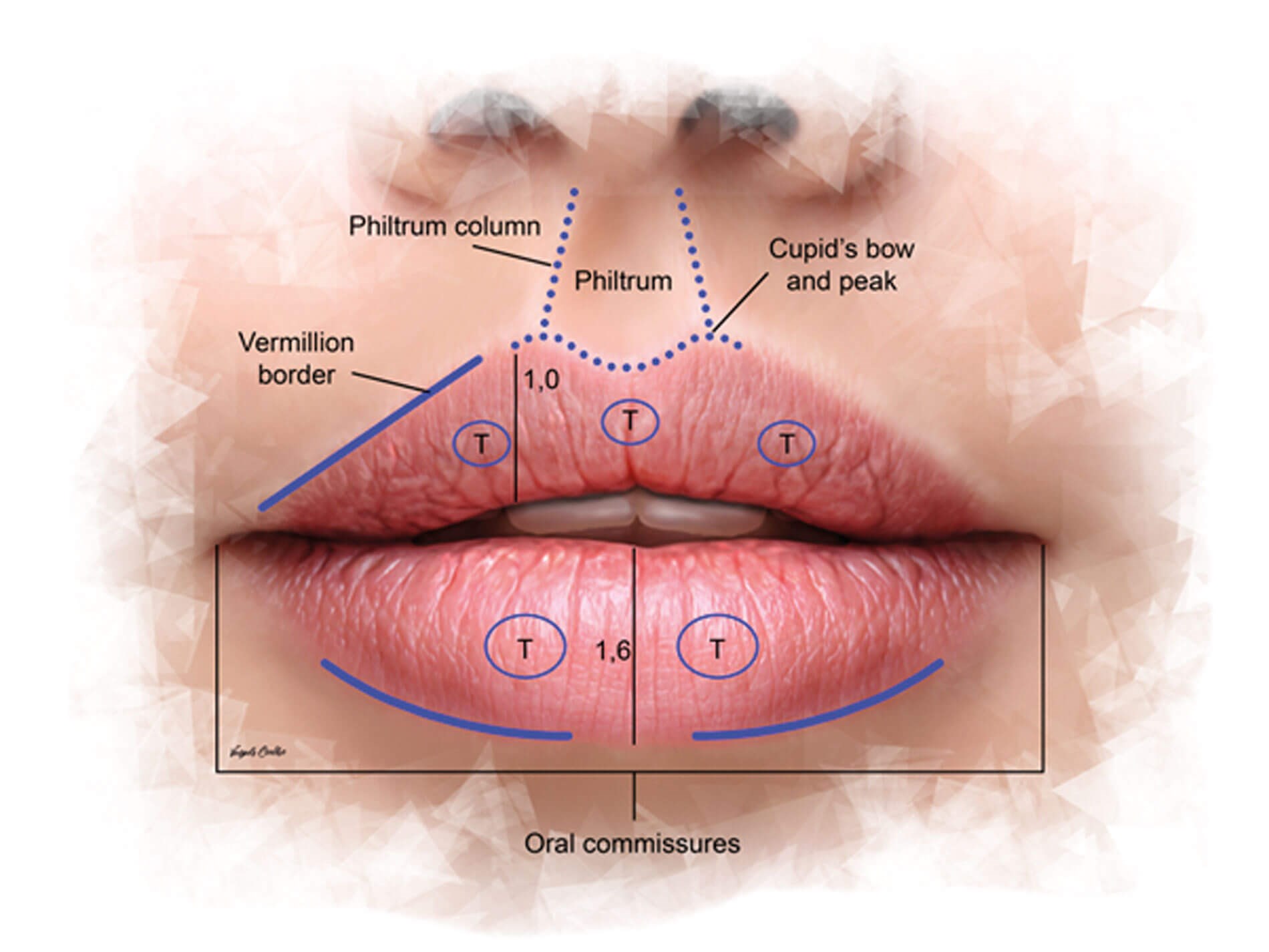
Figure 1: Surface anatomy of ideal lips and perioral area.
Surface anatomy of the ideal perioral area and lips
A youthful and attractive perioral area and lips should encompass the following anatomical landmarks (Figure 1):
- The upper cutaneous or white lip should be smooth, free from rhytides, with a central depression called philtrum.
- On profile view, the upper cutaneous lip is fairly short and concave.
- The philtrum is boundaried laterally by two divergent lines or ridges called ‘philtrum columns’, from the base of the nose to the clear and sharp Cupid’s bow and peak, located in the central area of the upper lip vermillion and cutaneous junction.
- The vermillion border should be a thin but well-defined line separating the red (vermillion body) from white (cutaneous) lip.
- The vermillion body or red lip is covered by a stratified squamous epithelium, which is in continuity with the oral mucosa of the gingivolabial groove. This specialised epithelium has some ‘wrinkles’ which should not be erased by lip enhancement procedures, they are the equivalent to our fingerprints.
- The red lip should be curved, with a reasonable height, full in the centre tapering towards the corners.
- These corners or oral commissures should be straight or slightly elevated from the central line of the lips, this should be curved accompanying the shape of the lips.
- Perioral framing of the lips should be smooth with no deflation and no static or expression wrinkles such as lines and melomental folds [2-4]
The presence of important subunits called ‘tubercles’ should not be overlooked. These are natural areas of dermal prominence, known to be embryological remnants of development and may be related to complex movements of the mouth by allowing extra surface area. They usually present as three on upper lip (one medial and two lateral) and two on lower lip [5].
Gender dymorsphism
A valuable point to understand the diversity of lip morphology is to appreciate gender dymorphism. There are fundamental differences, based on shape and form, between male and female lips that must be respected when performing treatments.
Male lips are usually flatter and wider, with less defined vermillion border, less accentuated Cupid’s bow and peak with a wider philtrum area. Often, some eversion with mild volume and projection are adequate to restore harmony. One should avoid producing exaggerated projection or definition, mainly of the central portion of the lips, to avoid feminisation, unless this is the purpose of the treatment.
A study from 2015 revealed that a full upper lip is an important feature of both feminine and masculine attractiveness, whereas a full lower lip might imply feminine attractiveness, but it does not play an important role in masculine appeal [6].
Ethnicity
It is also important to recognise the role of ethnicity; the clinician should not disregard the unique characteristics of ethnic patients, mostly seeking some enhancement opposed to changing their heritage features.
The golden ratio, also known as the Fibonacci ratio or ‘divine proportions’, is considered the standard for Caucasians, with a ratio of 1 to 1.6 for upper lip to lower lip height on frontal view, while in Black ethnicity this ratio is 1:1.
Wong et al. showed that Asian (Chinese and Korean subjects) groups exhibited notably different lip parameters and lip-projection volumes from that of Caucasians:
- Chinese women: mean upper to lower lip ratio of 1:1.25
- Korean women: mean upper to lower lip ratio of 1:1.11 [7]
- Lips are on-line or more retrusive in relation to the Ricket’s line
The Rickett’s line (drawn from the tip of nose to tip of chin) can be used as an imaginary line during pre-assessment, with ideal Caucasian lips not protruding the line, Black / African ethnicity with protruding lips and Asians on-line or retrusive to it. However, with retrogenic or prognathic chins, this is not an advisable assessment.
Lip size preferences are also variable, with Asians favouring smaller lips than Caucasians, and African-Americans preferring lips that are more protrusive on profile view compared to Hispanics and Japanese groups [8]. Appreciating the subtle differences between ethnic groups and implementing a more specific approach will lead to more natural results.
Ageing
Understanding the morphology of a youthful and balanced perioral area will help to recognise the disproportions and changes arising from the ageing process.
Similar to other facial areas, ageing of the perioral area is influenced by the coaction of the distinct layers: bone, ligaments, fat, muscles and skin and the intrinsic and extrinsic ageing factors such as genetics, hormonal changes, smoking, alcohol, UV exposure, nutrition, stress and general lifestyle, all leading to degradation of collagen and elastin. Onset and speed of age-related changes varies between each structure, individual, gender and ethnicity [9].
Iblher et al. used photometric analysis and cranial magnetic resonance imaging to show significant lengthening of the upper lip with thinning of the vermillion, decrease of incisor show and loss of anterior projection. They concluded that there was no volume loss on upper lip but caudal redistribution of soft tissue [10].
On the other hand, Tonnard et al. suggested that perioral ageing is affected by a combination of soft tissue lengthening, thinning and volume loss, and not tissue redistribution [11].
The main clinical changes in surface anatomy are:
- Elongation of cutaneous upper lip with flattening of philtrum and faded philtrum columns
- Upper red lip equally projected or posterior to lower lip
- Loss of definition of vermillion border and cupid’s bow and peak
- Downturn of oral commissures
- Presence of perioral rhytides
- Development of marionette lines / folds [12]
As a rule, the lower lip ages better than the upper, with wrinkles appearing at a later stage. Other characteristics are more noticeable with dynamic movements. Assessment should include photographs or videos with patients smiling, pulling down the corners of the mouth, tensing the chin and puckering lips, these would assist in recognising features such as muscle tonicity, degree of perioral lines, any asymmetry, smile line / arc, gingival display, buccal corridors and dental status. Dentition is a crucial aspect of pre-treatment evaluation, as missing teeth, crowding and malocclusion will negatively affect results.If recognising all the ageing features, one should be mindful that treatment will be challenging and a multimodal approach including dental referral and / or surgical intervention may have to be implemented.
Muscles of facial expression
Facial muscular anatomy has been defined for centuries with the corner of the mouth being one of the earliest anatomic regions described in detail [13]. The modiolus is a mobile and dynamic but dense fibromuscular point, located at the corner of the mouth. It is a salient structure in the movement of facial expressions, with no bone attachment and levelled by levator and depressor muscles.
Muscles joining at the modiolus:
- Orbicularis oris
- Zygomatic major
- Levator anguli oris
- Buccinator
- Risorius
- Depressor anguli oris
- Platysma
Knowledge of the levators and depressors is paramount for more customised procedures.
Levator muscles, joining the upper lip:
- Levator labii superioris alaque nasi (LLSAN)
- Levator labii superioris (LLS)
- Zygomatic minor
Depressor muscles, joining the lower lip:
- Depressor labii inferioris
- Mentalis
- Platysma
The orbicularis oris (OO) is a broad elliptical muscle, with no osseous origin but intertwined with fibres of other facial expression muscles. Currently accepted as consisting of two parts, an upper and lower part joined at the modiolus. Each part is composed of two distinct portions, resembling the letter ‘J’:
- Pars marginalis: located in the vermillion, gives the lips its curved shape and acts as a sphincter.
- Pars peripheralis: located in the cutaneous lips, straighter and it has a dilatory function [2,3].
Vascularisation
This is a pivotal part of the underlying anatomy of this area, at risk of adverse effects such as bleeding, bruising, haematomas and more severe complications as a result of vascular occlusion leading to skin necrosis, visual disturbances and blindness.
The facial artery (FA) is an extension of the external carotid artery (ECA) curving around the mandibular body in a very stable position, deep to platysma muscle and deep adipose tissues, medial to the anterior border of the masseter muscle, becoming more superficial as it travels medially to give off branches which will supply the perioral region:
- Superior labial artery (SLA) and septal, collumela and subalar branches for upper lip.
- Inferior labial artery (ILA), horizontal labiomental artery and vertical labiomental artery for lower lip
Cotofana et al. in a large multicentre anatomical study identified three different distribution patterns of SLA and ILA:
- Submucosal, between the OO muscle and oral mucosa: 78.1%.
- Intramuscular, between the superficial and deep layers of the OO muscle: 17.5%.
- Subcutaneous, between the skin and OO muscle: 2.1% (Figure 2)
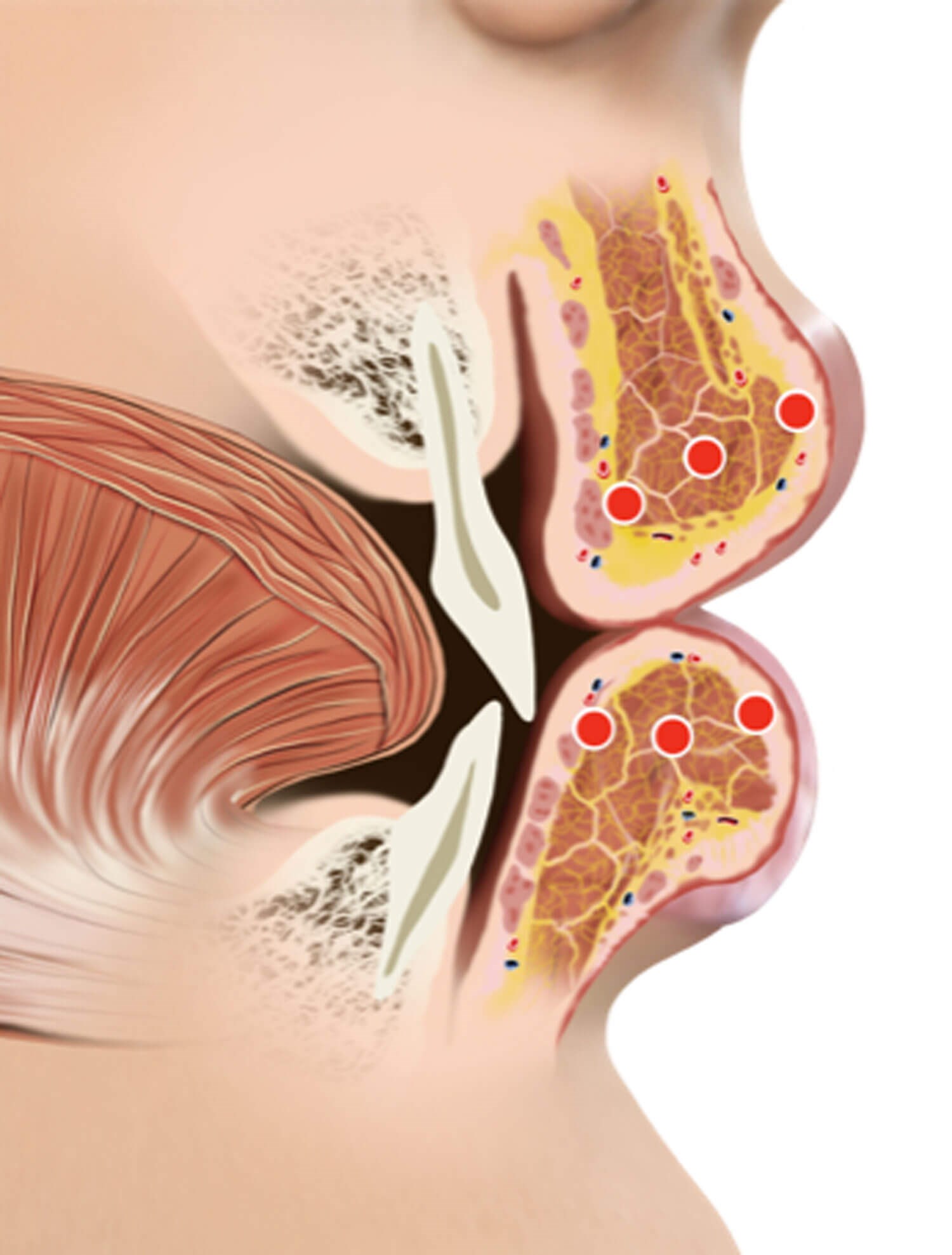
Figure 2: Position of the labial arteries: subcutaneous, intramuscular and submucosal.
These results corroborate previous views that injections should be performed in the more superficial plane [14,15]. Furthermore, this study revealed the variability in the position of the arteries, changing planes during their course, with 29% for the SLA and 32% for the ILA [16].
Additional clinically relevant information on the three-dimensional (3D) route of the SLA and ILA within the lips was demonstrated by using ultrasound imaging:
- The depth of the SLA in the upper lip was 5.6 ± 0.13mm and of the ILA in the lower lip was 5.2 ± 0.14mm.
- Both arteries were more frequently located within the red lip than in the cutaneous lip: upper lip (83% vs. 18.7%) and lower lip (86.2% vs. 13.8%).
- In the midline, the artery was present in 100% of the cases
This suggested that a perpendicular approach (from the cutaneous lip) may be safer due to the horizontal course of the arteries allowing for a reduced contact area and the most frequent location within the red lip [17].
Techniques injecting small amounts of filler into the superficial intramuscular plane to achieve lip eversion and deeper intramuscularly to expand the vermillion zone have been proposed, indicating the presence of a ‘safer area’ even at deeper planes [18].

Figure 3: Before and after perioral treatment with HA dermal fillers (Stylage® range, Vivacy Paris).
Areas treated: perioral wrinkles, nasolabial and marionette folds, oral commissure and labiomental crease.

Figure 4: Before and after treatment of lips with multiple injection techniques at subcutaneous /
superficial layer, using cannula and needles. Product: Stylage® Special Lips, Vivacy Paris.
Nevertheless, from a technical perspective, injections in more the superficial plane accompanied by judicious selection of product (correct rheological properties), gentle and well-suited techniques (low pressure, slow injection, appropriate for the diagnosed issue) and the use of a familiar instrument (cannula and / or needle), will contribute to the end goal of safer and more natural results (Figures 3 and 4).
Conclusions
- Understanding of youthful characteristics and awareness of diversity in lip and perioral morphology attributed to age, gender and ethnicity is essential in promoting natural results.
- There is a high degree of variability in course and presence of these arteries, with both SLA and ILA following a tortuous course, with both changing layers throughout their route.
- Despite attempts to ascertain the safest technique for lip and perioral enhancement, knowledge of anatomy supported by statistics can only guide clinicians on how to undertake these procedures but will not eliminate the danger of vascular compromise as there is no ‘risk-free’ zone for facial injections.
- A critical approach regarding literature methodology is required as this may impact the outcome of some studies, especially in respect to anatomy specimens and their consistency
References
1. ASPS. Inaugural ASPS Insights and Trends Report: Cosmetic Surgery 2022.
https://www.plasticsurgery.org/
documents/News/Trends/2022/trends
-report-cosmetic-surgery-2022.pdf
[last accessed 4 July 2023].
2. Pirayesh A, Bertossi D, Heydenrych I. Aesthetic Facial Anatomy Essentials for Injections (1st ed.) London, UK; CRC Press: 2020.
3. Azib N, Charrier J-B, Cornette de Saint Cyr B, et al. Anatomy and Lip Enhancement. Paris, France; E2e Medical Publishing: 2011.
4. Carey JC, Cohen MM Jr, Curry CJ, et al. Elements of morphology: standard terminology for the lips, mouth, and oral region. Am J Med Genet A 2009;149A(1):77-92.
5. Harris S, Alfertshofer M, Allen R, et al. Introduction of the Lip Classification of Tubercles: A Novel Approach to Minimally Invasive Aesthetic Lip Treatments. Aesthet Surg J Open Forum 2023;5:ojad007.
6. Penna V, Fricke A, Iblher N, et al. The attractive lip: A photomorphometric analysis. J Plast Reconstr Aesthet Surg 2015;68(7):920-9.
7. Wong WW, Davis DG, Camp MC, Gupta SC. Contribution of lip proportions to facial aesthetics in different ethnicities: a three-dimensional analysis. J Plast Reconstr Aesthet Surg 2010;63(12):2032-9.
8. Heidekrueger PI, Szpalski C, Weichman K, et al. Lip Attractiveness: A Cross-Cultural Analysis. Aesthet Surg J 2017;37(7):828-36.
9. Cotofana S, Fratila AA, Schenck TL, et al. The Anatomy of the Aging Face: A Review. Facial Plast Surg 2016;32(3):253-60.
10. Iblher N, Stark GB, Penna V. The aging perioral region -- Do we really know what is happening?. J Nutr Health Aging 2012;16(6):581-5.
11. Ramaut L, Tonnard P, Verpaele A, et al. Aging of the Upper Lip: Part I: A Retrospective Analysis of Metric Changes in Soft Tissue on Magnetic Resonance Imaging. Plast Reconstr Surg 2019;143(2):440-6.
12. Tonnard PL, Verpaele AM, Ramaut LE, Blondeel PN. Aging of the Upper Lip: Part II. Evidence-Based Rejuvenation of the Upper Lip-A Review of 500 Consecutive Cases. Plast Reconstr Surg 2019;143(5):1333-42.
13. Pessa J, Rohrich R. Facial Topography: Clinical Anatomy of the Face. London, UK; CRC Press: 2012.
14. Tansatit T, Apinuntrum P, Phetudom T. Cadaveric Assessment of Lip Injections: Locating the Serious Threats. Aesthetic Plast Surg 2017;41(2):430-40.
15. Lee SH, Gil YC, Choi YJ, et al. Topographic anatomy of the superior labial artery for dermal filler injection. Plast Reconstr Surg 2015;135(2):445-50.
16. Cotofana S, Pretterklieber B, Lucius R, et al. Distribution Pattern of the Superior and Inferior Labial Arteries: Impact for Safe Upper and Lower Lip Augmentation Procedures. Plast Reconstr Surg 2017;139(5):1075-82.
17. Cotofana S, Alfertshofer M, Schenck TL, et al. Anatomy of the Superior and Inferior Labial Arteries Revised: An Ultrasound Investigation and Implication for Lip Volumization. Aesthet Surg J 2020;40(12):1327-35.
18. Trévidic P, Criollo-Lamilla G. French Kiss Technique: An Anatomical Study and Description of a New Method for Safe Lip Eversion. Dermatol Surg 2020;46(11):1410-7.
Declaration of competing interests: The author is an International Key Opinion Leader for Vivacy UK. She has not received any honorarium or reimbursement for writing this article.
COMMENTS ARE WELCOME








