
Polydioxanone (PDO) threads summary:
- Colourless, crystalline, biodegradable synthetic polymer
- Monofilament
- Biodegradation by hydrolysis
- Mainly urine excretion
- Absorption rate 180 days
- Breaking strength 53% at 42 days
- Long established safety record in general surgery as a suture material (PDS II Ethicon)
- PDO (Korea) = PDS II (Ethicon)
- 2011: Non-barbed 6-0 thread in 29G needle approved by the Korean FDA for lipolysis, neo-vascularisation and collagen regeneration.
Postulated mechanism of action is two-fold
- Mechanotransduction (acupuncture effect) – ability of the cell to sense, process and respond to mechanical stimuli [1].
- Wound contraction – foreign body reaction, wound healing, fibrosis, contraction [2], fibrous bridging.
Barbed thread comparison
The three-dimensional (3D) spiral multi-directional 2-0 barbed thread offers more tissue anchoring than the ordinary non-spiral multi-directional 2-0 barbed thread. Both threads are inserted with a blunt cannula.
Pre-treatment procedure
- Consultation and obtain informed consent.
- Photographs are essential to demonstrate existing asymmetry.
- Contraindications the same as for any aesthetic procedure, eg. HA fillers, etc.
- Prophylactic antibiotics: azithromycin 500mg two hours pre-treatment offers high blood concentrations, followed by 500mg daily for two days.
- Aseptic technique: apply a cap to contain hair, apply tape over hair line, cleanse treatment area with 70% surgical spirits or chlorhexidine, sterile folio drape.
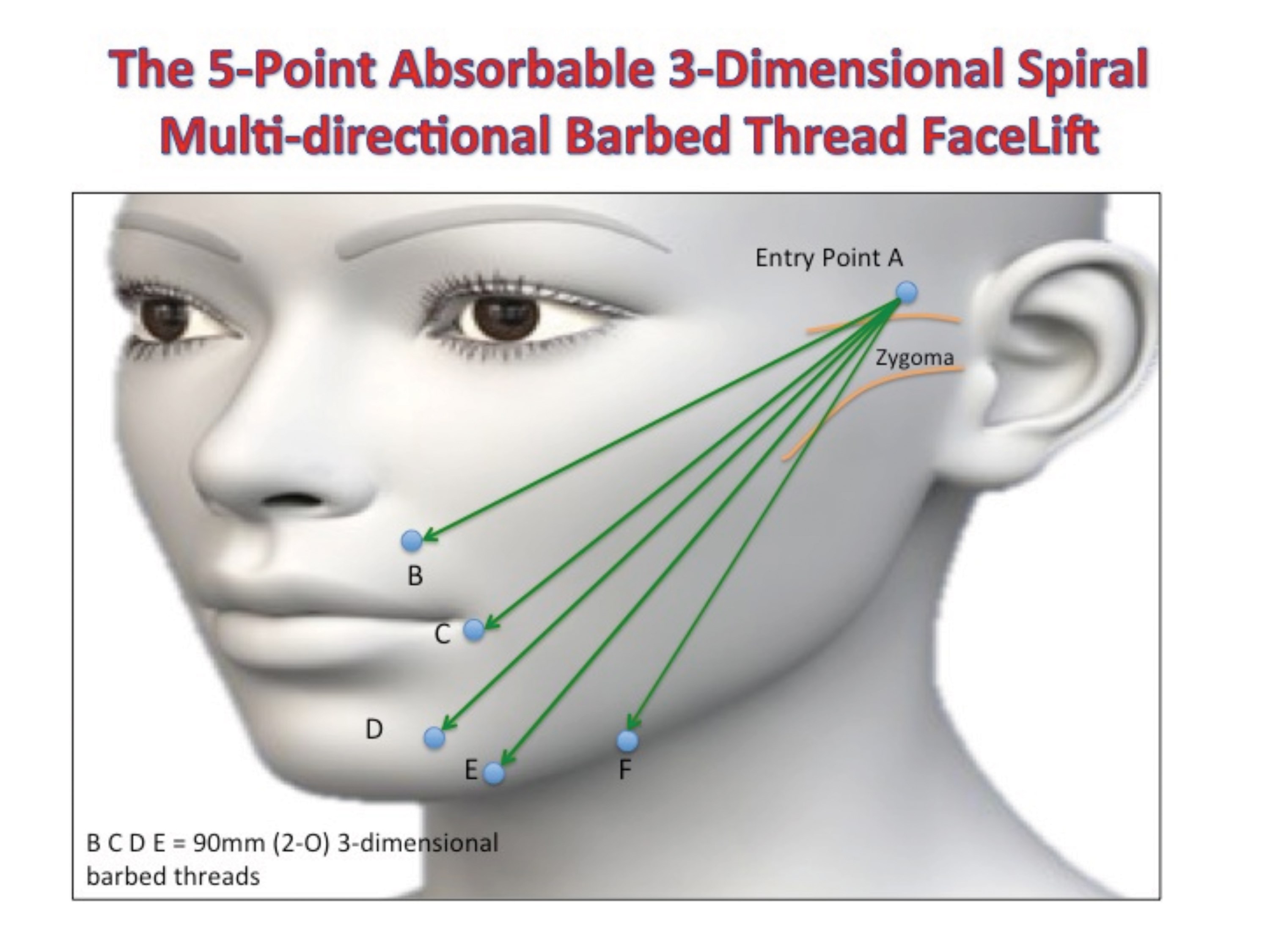
- Mark the treatment area with a marker pencil: connect entry point A to end points B (naso-labial fold), C (2cm lateral to corner of the mouth), D (through marionette line), E (marionette/mandible) and F (mid-jowl).
Insertion technique
a. Anaesthesia: end points – intra-oral infra-orbital nerve block with 0.5ml 3% lignocaine and intra-oral mentalis nerve block with 0.5ml 3% lignocaine. Entry point – dermal and sub-dermal local infiltration with 1.0ml 2% lignocaine plus adrenaline 1:200,000.
b. Puncture the skin of the entry point with a 16-gauge needle and subcise the subcutaneous tissue up to 1.5cm from the skin entry point.
c. Aspirate 1.0ml of 3% lignocaine into a 1.0ml Luer Lok syringe and pass the end of the thread through the end of the syringe before the cannula is connected to the syringe. The 1.0ml syringe now acts as a handle (Dr Irfan Mian’s technique).
d. Insert the tip of the cannula bevel up slowly through entry point A in the level of the subcutaneous tissue (connective tissue) towards end point B. In the event of any discomfort, stop insertion of the cannula and inject 0.1ml lignocaine, wait for about 20 seconds and continue to insert the cannula.
e. When end point B is reached, place two fingers (index and middle) over the tip of the cannula and turn the cannula twice (clockwise or anti-clockwise).
f. Maintain pressure on the cannula tip and slowly withdraw the cannula whilst following the tip of the cannula with the two fingers and simultaneously applying pressure on the thread.
g. Remove the cannula completely and connect a clamp or artery forceps to the end of the protruding thread.
h. Repeat the process for threads C, D E and F.
i. Clamp all five threads together, apply gentle tension and turn them five to eight times.
j. Cut the threads short in order to ensure submersion under the skin.
k. Cleanse the entry point with alcohol, apply Bactroban antibiotic cream / ointment and cover with steri-strips or a small plaster.
Post-treatment procedure
- Paracetamol for discomfort. No non-steroidal anti-inflammatory drugs (NSAID).
- Avoid prolonged opening of the mouth for two weeks (no dental appointments).
- Abstain from alcohol, extreme heat (sauna) and exercise for seven days.
- Follow-up photographs at one month, end point at four months.
- Consider maintenance treatments every 12-18 months.

Patient aged 43 years: left – before procedure and right – three months after.
Side-effects and complications
- Swelling and minor bruising at insertion point.
- Thread migration and protrusion if not cut short enough at entry point.
- Nerve trauma if insertion level is too deep.
- Vascular trauma minimal due to blunt cannula.
- Infection is rare.
- Sharp pulling pains during first two weeks.
- Asymmetry.
- Visible threads when inserted too superficially.
- Epidermal granuloma and scar tissue at insertion point.
References
1. Langevin HM, Bouffard NA, Badger GJ, et al. Subcutaneous tissue fibroblast cytoskeletal remodelling induced by acupuncture: evidence for a mechanotransduction-based mechanism. J Cell Physiol 2006;207:767-74.
2. Gabbiani G, Hirschel BJ, Ryan GB, et al. Granulation Tissue as a Contractile Organ. A study of structure and function. J Exp Med 1972; 135(4):719-34.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME







