
It is reasonably easy for the medical professional to underestimate the impact of appearance on a patient’s quality of life. Sun-tanned skin is viewed as healthy and desirable, and overseas vacations offer almost guaranteed sunny days. Paradoxically, prematurely aged skin is seen as unattractive by patients and their friends and colleagues, resulting in a negative effect on self-image.
While many patients are keen to point out that they always use sun-protection, the amount used is generally insufficient, and many still use no protection while at home. Most of my patients therefore present with some degree of sun-damage, as overexposure to ultraviolet light causes damage to cells, vessels and connective tissue leading to a proliferation of vessels, dyspigmentation, sallow skin and irregular pore size. While sun-damage can affect any exposed area, the area most continually exposed, and most scrutinised, is the face.
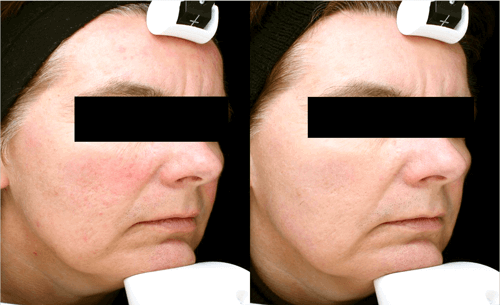
Before and after photos of patient treated for sun-damaged skin.
Nordlys is a multiplatform system, consisting of narrowband intense pulsed light (IPL) handpieces, a long-pulsed Nd:YAG (1064nm) and a fractional 1550nm wavelength diode laser. All have a role in rejuvenation of the face, and the device is indicated for photorejuvenation, skin texture, treatment of epidermal pigment, and telangiectasias. Both Nd:YAG and IPL target chromophores in the skin. And with Nordlys, I can choose an appropriate waveband and pulse length for each chromophore.
Improvement in skin texture arises from post-treatment collagen breakdown and replacement following secretion of matrix metalloproteinase-1 (MMP-1), transforming growth factor-β1 (TGF-β1), and the mitogen-activated protein kinase (MAPK) in fibroblasts.
The procedure
This starts with an initial interview to discuss patient concerns and offer a timescale for resolution. Most patients present with sun-damaged skin that is principally vascular in nature, or principally pigment related, or a mixture of both. For all groups the face must be clean and free of make-up, before a thin layer of optical coupling gel is applied.
If there is any dyspigmentation, I start the whole face with the 555‑950nm waveband, using the standard 48mm x 10mm spot. A default fluence is suggested by the device, based on Fitzpatrick skin type and level of suntan. The default is generally sufficient for treating bony or sensitive areas, but can be increased on fleshier areas, based on skin reaction and client sensitivity. The clinical effect is rapid for skin types I and 2 – within a minute or so of the energy being delivered to the skin any epidermal pigment starts to darken because of photo-oxidisation, and this darkening continues for some hours leading to an appearance of coffee-grounds on the skin.
If the patient shows only diffuse redness prevalent in skin types 1-2, I choose a 530-750nm waveband. This has a higher uptake by haemoglobin as the waveband includes the 542nm haemoglobin absorption peak, but also has a greater absorption in melanin. I prefer to use it on lighter skinned patients, and one month after a treatment has removed excess pigment. Treatment is again quick, the clinical endpoint is a temporary blueing of the vessel, lasting only a few seconds. Small areas of individually visible vessels can be treated immediately after diffuse redness, using a pulse based on the size of the vessel. Deeper telangiectasias, or those placed inconveniently on the nostrils or alar fold, can be treated with Nd:YAG.
Conclusion
The above treatments can be used for prophylactic care to prevent the visible reappearance of sun-damage or be combined with fractional laser treatment (skin resurfacing) to further improve skin texture and reduce rhytids, giving instant gratification in terms of pigment and vessels followed by a slower neocollagenesis.
Declaration of competing interests: The author has been reimbursed by Syneron-Candela, the manufacturer of Nordlys, for presenting at IMCAS 2019.
COMMENTS ARE WELCOME



