
With the advent of hyaluronic acid fillers, safe and effective non-surgical facial rejuvenation has been advanced. Hyaluronic acid fillers are becoming increasingly popular amongst patient who seek facial enhancement. In 2013, there were over 1.8 million treatments using hyaluronic acid performed in the US alone, representing a 31% increase from the previous year [1]. Fillers are placed in the dermis using needles in order to improve the appearance of wrinkles, soften folds or hydrate the skin.
When fillers are placed in deeper planes, using needles or cannulae, there are many possibilities for facial rejuvenation and beautification. These include the enhancement of bony features, facial shaping and the lifting of soft tissues. The ability of a treatment that uses hyaluronic acid fillers to make a patient appear more attractive, more youthful or refreshed, depends on the operators understanding of the ageing process, aesthetic ideals and proper patient assessment.
The need for volume
Ageing affects the soft and hard tissues of the face. It is primarily an involutional process, rather than a gravitational one [2]. The bony skeleton, deep and superficial fat compartments of the face deflate over time [3]. As the mandible, zygoma and periorbital bones resorb, structural support for the soft tissues of the jawline, midface, and brows lessens and ptosis becomes apparent. The deep and superficial fat compartments of the face also atrophy asynchronously, such that various hollows, grooves and shadows appear as one ages. The relative resistance of nasolabial and jowl fat to atrophy exacerbates the nasolabial grooves and jowls as the fat in the midface and elsewhere disappears. Therefore, a pseudoptosis of the nasolabial fat and jowls due to volume loss, rather than excess, occurs. Attenuation of facial ligaments and deterioration in the quality of the skin through intrinsic and extrinsic ageing compound these signs. The involutional and atrophic changes that occur with ageing in the face are ameliorated using fillers (Figure 1). The strategy for facial contouring with fillers begins with an assessment using inspection and facial imaging.
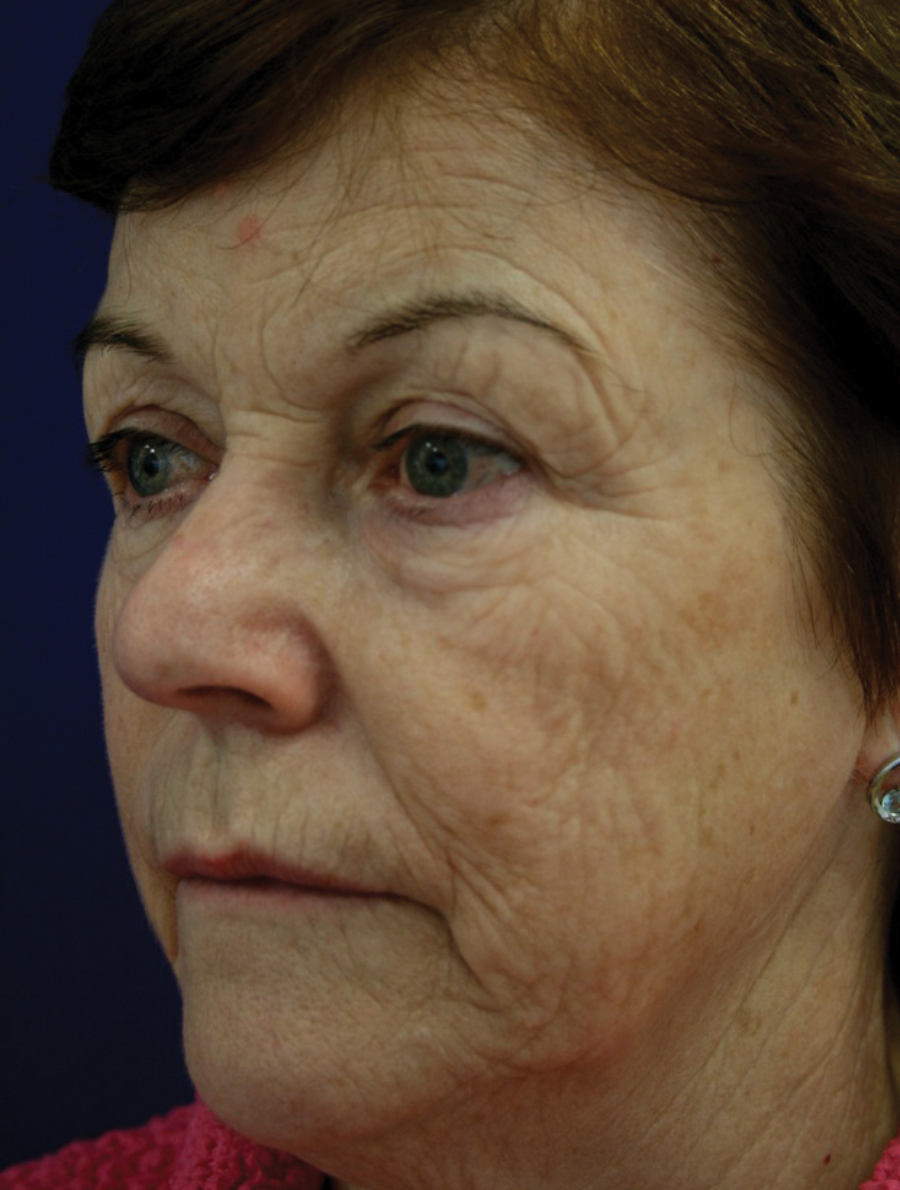

Figure 1: a) Before and b) after diffuse volume restoration with hyaluronic acid fillers combined with laser resurfacing for photoaging. (Courtesy of Dr Peter Predergast@)
Facial assessment
Upon immediate inspection, a general idea of the age and health of the patient can be ascertained. It is easy to identify facial volume loss: shadows at the lid-cheek junction, flattened midface, temporal shadowing and a small or receding chin with jowling. The author utilises the Vectra 3D M3 system (Canfield Scientific Inc. Fairfield NJ) to generate a high-resolution image of the patient’s face (Figure 2). The three-dimensional image obtained is used to highlight and to educate the patient in the role of volume in facial ageing. The imaging software allows manipulation of the image and simulation of various cosmetic procedures, including volume restoration and contouring using fillers. Patients are more accepting of panfacial volume restoration when they see the results that might be achieved.

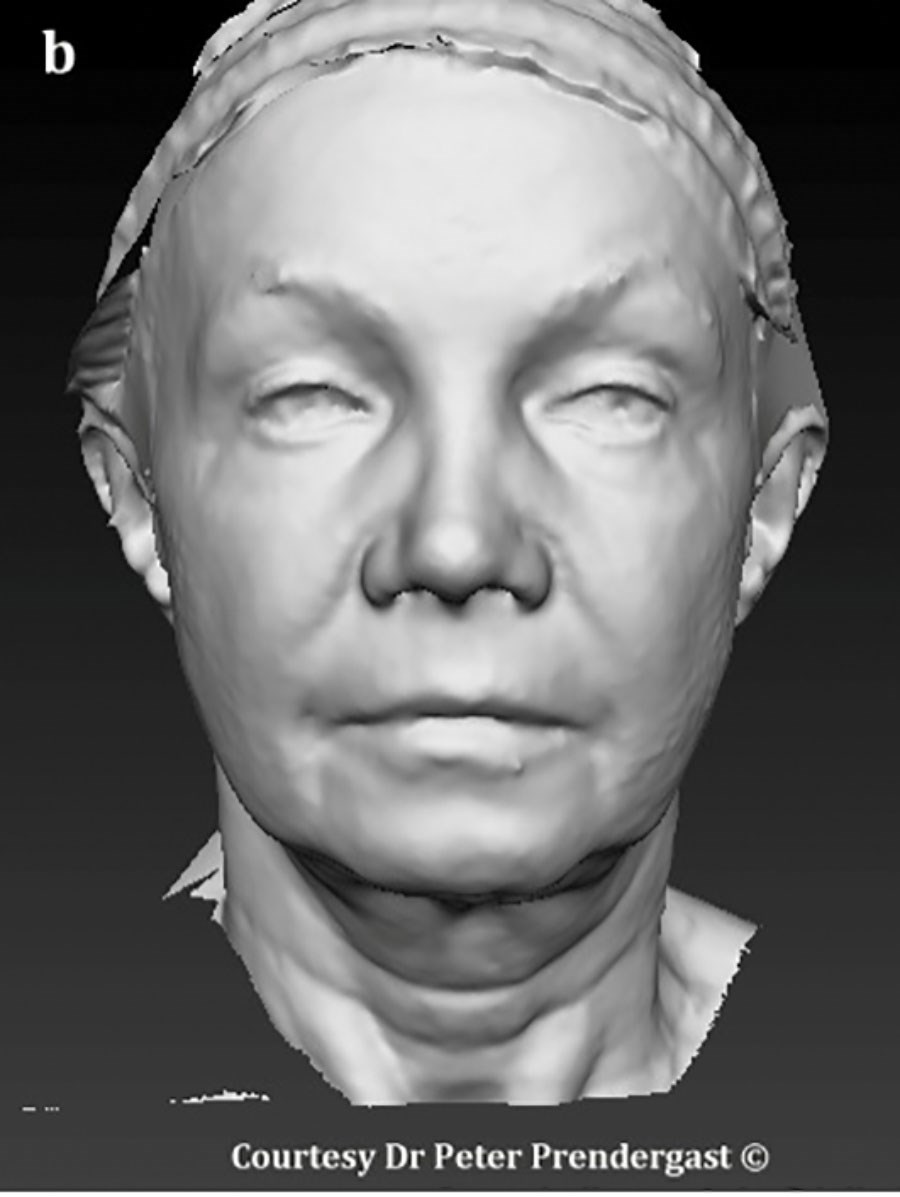


Figure 2: a) Pre-treatment image capture using Vectra 3D M3 (Canfield Scientific Inc. Fairfield NJ); b) Gray tool using same image that allows volume assessment; c) same patient before and d) after mid- and lower face volume restoration with hyaluronic acid fillers.
Aesthetic ideals
The hallmark of a youthful face is appropriate facial volume or fat and seamless smooth transitions between the various units of the face. In females, the midface should be adequately full with tapering over the defined jawline toward the chin. The most projected point of the midface, the cheekbone point or zygomaxillary point, lies 20-25mm below and slightly lateral to the lateral canthus. The lid-cheek junction should be smooth and difficult to identify. The jawline should be defined and the lower lip and chin should be twice the height of the upper lip. There may be a shadow created by the prominence of the zygomatic arch, but a shadow created by skeletonisation around the superior temporal crest is undesirable. In men, more prominence of the bony features is acceptable.
“The hallmark of a youthful face is appropriate facial volume or fat and seamless smooth transitions between the various units of the face.”
Pertinent anatomy
Regional nerve blocks are useful before panfacial volume restoration using fillers [4]. The infraorbital nerve exits its foramen just medial to the mid-pupillary line 8-10mm below the orbital margin. The foramen is oriented inferomedially, so cannulae should approach this area from laterally to avoid inadvertent injection directly into the foramen when placing filler preperiosteally. A small aliquot of anaesthetic placed over the periosteum just inferior and lateral to the orbital margin blocks the zygomaticofacial nerve before cheek enhancement without obscuring the anatomy unduly. The mental nerve is blocked from an intraoral approach, placing anaesthetic just below the mucosa at the root of the second lower premolar tooth. Knowledge of the vascular anatomy of the face, and the presence of rich internal-external carotid anastomoses is important before injecting fillers for facial contouring. Inadvertent intravascular injection, particularly in the glabellar area, can lead to blindness [5]. The orbicularis retaining ligament tethers orbicularis oculi and contributes to the shadow of the tear trough. The zygomaticocutaneous ligament further divides the cheek and interrupts the smooth contours of the midface, particularly when there is fat loss. Fillers lift and project soft tissues like a balloon re-inflating and can efface many of these contour irregularities (Figure 3).


Figure 3: a) Volume loss in the midface produces shadows and is exacerbated by the tethering effect of the orbicularis retaining ligaments and zygomaticocutaneous ligaments; b) after placement of hyaluronic acid fillers at the lid-cheek junction and midface, the shadows are effaced.
Technique
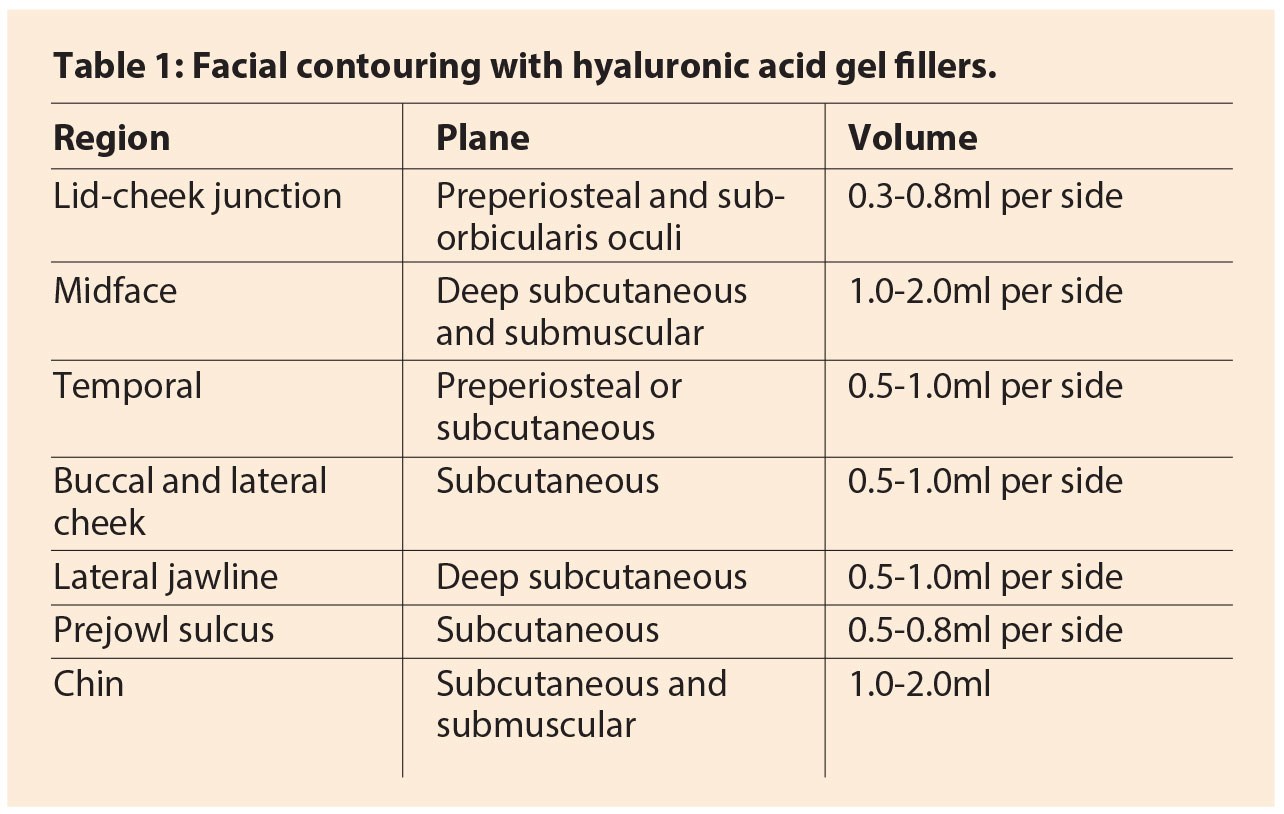
The technique of contouring the face using fillers depends on the indication. Fillers may be used to restore diffuse volume loss, smooth junctions, project and lift tissues and define features. The author utilises hyaluronic acid fillers almost exclusively for several reasons. Firstly, they are non-permanent. This allows a tailored approach over time as the facial shape and volume change with age. Secondly, the broad product range allows different products to be used in each area: softer less viscous fillers under the thin skin and muscle of the infraorbital area, more viscous products with higher lifting capacity in the cheeks and jawline. Finally, hyaluronic acid fillers can be quickly removed with the use of hyaluronidase. Although rarely necessary, it is reassuring to know the product can be removed in the event of a complication or dissatisfied patient. A guide to planes and volumes in facial contouring using fillers is provided in Table 1.
Diffuse volume loss
Where there is diffuse volume loss, the patient may present with hyperdynamic lines throughout the face as the skin almost sits on the underlying mimetic muscles. Laying down a blanket of hyaluronic acid filler beneath the dermis lifts the skin and provides a buffer between the skin and muscle (Figure 1). Long 25-gauge cannulae are ideal for this purpose. The filler is inserted in the subcutaneous plane using the fanning technique through strategically placed entry sites. Filler is placed throughout the lateral face from the zygomatic arch inferiorly across the buccal area to the jawline. Resistance is felt as the cannula passes through the dense fibrous septae in the preauricular area. About 1-2ml is usually required on each side to lift the skin and efface the hyperdynamic cheek lines.
Junctions
The most important, and sometimes the most challenging, area to contour for rejuvenation is the lid-cheek junction. Medially, the lid-cheek junction appears as the so-called tear trough, a darkened groove that extends inferolaterally from just below the medial canthus. First, the author performs an infraorbital nerve block using 0.4ml 2% xylocaine (lidocaine with 1:200,000 epinephrine) injected transdermally. This provides adequate vasoconstriction after 12 minutes as well as complete anaesthesia. Then very small aliquots (0.02-0.05ml) of cross-linked hyaluronic acid are placed preperiosteally along the groove. This continues along the lid-cheek junction from medial to lateral. A needle provides accuracy over the periosteum, whereas a 27-gauge cannula may be used to place tiny strands of filler just beneath orbicularis oculi. Usually 0.5-1.0ml in total is adequate per side. During the procedure, the patient is asked to gaze upwards intermittently to assess the depth of the groove which becomes more pronounced in upward gaze as orbital fat bulges over the orbital margin against the thin orbital septum.
In order to improve the temporal hollow and reduce the shadow created posterior to the temporal crest line, volume is required in the temporal area. This can be placed either on the periosteum or in the subcutaneous plane. In thin patients, a robust hyaluronic acid gel is placed on the periosteum using 5-8 aliquots to lift the temporalis muscle. In less skeletonised patients, a soft hyaluronic acid filler is placed subcutaneously using the fanning technique with a cannula, taking care to avoid ridges. The temporal branch of the facial nerve passes within the superficial temporal fascia between these two planes.



Figure 4: Planning facial volume restoration with fillers. a) Before – there is flattening of the midface and the jawline is poorly defined. b) Areas amenable to placement of hyaluronic acid fillers: light blue, palpebromalar junction or groove; dark blue, soft tissues over midface, zygomaxillary point and cheekbones; purple, buccal area and lateral face; orange, pre-jowl sulcus and angle of mandible; green, chin; yellow, temporal hollow. The red points represent entry points for cannulae. Note the avoidance of filling over the nasolabial and jowl fat pads. c) After volume restoration. The malar area is projected creating a more pleasing ogee curve, and the jawline appears stronger.
Midface
In women, filler is placed in the deep medial cheek fat just lateral to the nasolabial fat pad to enhance the midface and smooth the transition between the lower lid and the cheek. The filler is placed using the fanning technique with a long 22-gauge cannula, from medial to lateral. Care is taken to ensure the cannula is below orbicularis oculi as the tip approaches the orbital rim. The latter is protected with the index finger of the non-injecting hand. More volume is placed below and lateral to the lateral canthus to enhance the zygomaxillary point and create an attractive ogee curve. A second cannula entry point is made near the hairline over the lateral aspect of the zygomatic arch. Filler is placed subcutaneously and submuscularly to enhance the cheekbones, blend with the medially placed volume, and provide projection and lifting of the midface (Figure 4). About 2-3ml of filler per cheek is sufficient to deliver good results. In men, the focus is on enhancing the bony zygoma and zygomatic arch rather than filling the medial cheek fat. As a general rule, cheek enhancement and projection require volume to be placed above an imaginary line from the oral commissure to the tragus, concentrating on the cheekbone point, blending with the infraorbital volume, and feathering over the cheekbone. Patient preference determines whether the cheekbones are significantly enhanced or not. Some patients request high or prominent cheekbones.
Jawline
Bony resorption in the mandible, ptosis of the jowl fat pad, and involution of the chin fat pad all contribute to a poorly defined jawline. Non-surgical correction using fillers is an attractive option for patients who cannot afford downtime. The author places filler at the angle of the mandible and in the pre-jowl sulcus using a single entry point with a 22-gauge cannula. The volume required is determined by the degree of volume loss along the jawline. The pre-jowl sulcus, posterior jawline and chin may require 4.0ml (Figure 4).
Surface
Dermal fillers complement facial contouring with fillers and should be performed immediately after the deeper volume has been placed. These include filling the nasolabial folds, perioral lines, lip borders and marionette lines. Finally, hyperdynamic lines are addressed using botulinum toxin in the glabella, frontalis, orbicularis oculi, orbicularis oris and depressor anguli oris. To treat fine lines and photoageing, the author complements facial contouring with fractionated CO2 laser skin resurfacing.
References
1. American Society of Aesthetic Plastic Surgery statistics 2013; www.surgery.org
2. Kahn DM, Shaw RB. Overview of current thoughts on facial volume and aging. Facial Plast Surg 2010;26(5):350-5.
3. Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg 2008;121(6):2107-12.
4. Prendergast PM: Local regional anaesthesia. In: Prendergast PM, Shiffman MA. Aesthetic Medicine. Art and Techniques. Springer-Verlag Berlin Heidelberg; 2011.
5. Lazzeri D, Agostini T, Figus M, et al. Blindness following cosmetic injections of the face. Plast Reconstr Surg 2012;129(4):995-1012.
Declaration of competing interests: None declared.
COMMENTS ARE WELCOME


